Quinlan Taryn A G, Schroeder Brock, Kwon Sue, Barlow Jane F, Sherman Michael S, Anderson Heather D, Wright Garth, McQueen R Brett
Department of Health Systems, Management and Policy, University of Colorado Anschutz Medical Campus, Aurora, CO, USA.
Illumina, Inc., San Diego, CA, USA.
Pharmacoecon Open. 2021 Sep;5(3):449-458. doi: 10.1007/s41669-021-00261-y. Epub 2021 Mar 10.
Harvard Pilgrim Health Care expanded coverage for non-invasive prenatal testing (NIPT) to include all pregnant, single-gestation women aged < 35 years, through a performance-based risk-sharing (PBRS) agreement with Illumina to offset costs from coverage expansion. NIPT analyzes cell-free DNA fragments from a maternal blood sample to screen for fetal aneuploidies and is considered a more accurate screening method than conventional serum biochemical screening and nuchal translucency ultrasound-based approaches.
This study assessed the impact of NIPT coverage expansion on prenatal screening strategies and payer expenditures.
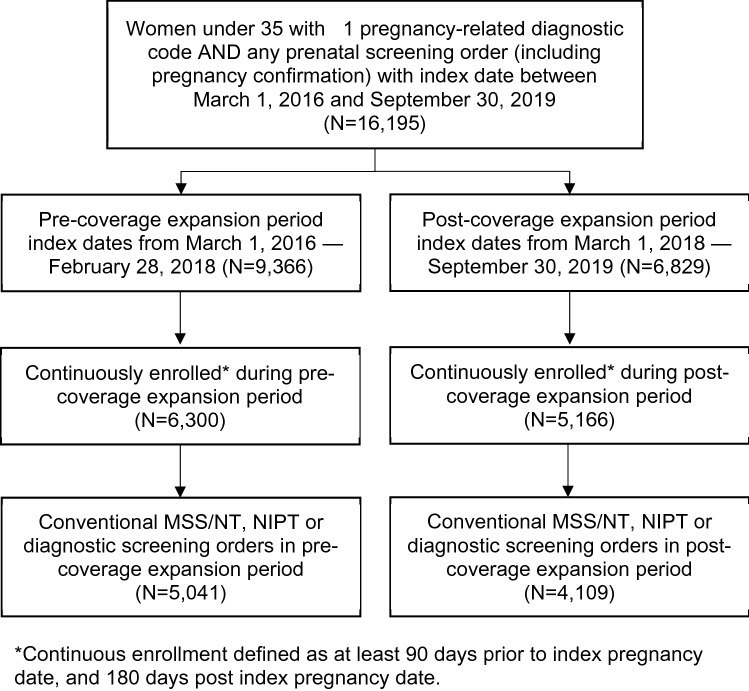
This was a real-world comparison of utilization and expenditures of prenatal screening and diagnostic testing in pregnant women aged < 35 years pre- (1 March 2016-28 February 2018) and post- (1 March 2018-30 September 2019) coverage expansion. Incidence rate ratios (IRRs) with 95% confidence intervals (CIs) were estimated to compare changes in utilization of conventional and NIPT-based prenatal screening methods. Change in per member per month (PMPM) expenditures in $US year 2020 were assessed post-coverage expansion using a budget impact model.
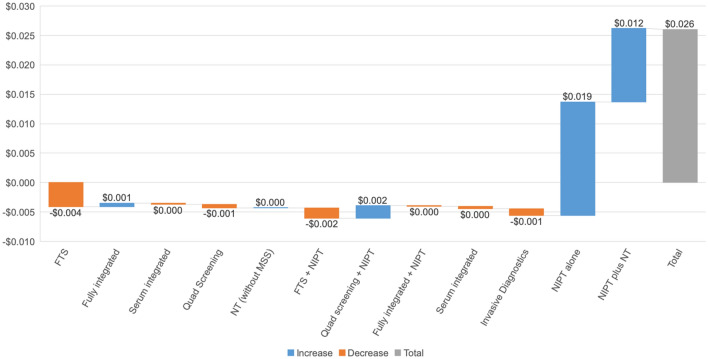
A total of 5041 and 4109 distinct pregnancies were identified in pre- and post-coverage expansion periods, respectively. Mean ± standard deviation maternal age was consistent between pre- and post-coverage expansion periods (30.35 ± 3.35 and 30.33 ± 3.28, respectively). Screening orders for conventional methods decreased, with an adjusted IRR in the post-expansion period of 0.87 (95% CI 0.85-0.90) times the rate in the pre-expansion period; orders for NIPT increased, with an adjusted IRR in the post-expansion period of 1.41 (95% CI 1.32-1.51) times the rate in the pre-expansion period. Invasive diagnostic testing was low at baseline (1.0%) and did not change post-coverage expansion. The change in PMPM is estimated at $US0.026 post-coverage expansion.
The PBRS agreement to expand NIPT coverage for women aged < 35 years was associated with an increase in NIPT utilization, decreases in conventional screening methods, and a modest increase in PMPM expenditures.
哈佛朝圣者医疗保健公司通过与Illumina签订基于绩效的风险分担(PBRS)协议,扩大了非侵入性产前检测(NIPT)的覆盖范围,将所有年龄小于35岁的单胎妊娠孕妇纳入其中,以抵消覆盖范围扩大带来的成本。NIPT分析母血样本中的游离DNA片段,以筛查胎儿非整倍体,被认为是一种比传统血清生化筛查和基于颈部透明带超声的方法更准确的筛查方法。
本研究评估了NIPT覆盖范围扩大对产前筛查策略和支付方支出的影响。
这是一项对年龄小于35岁的孕妇在覆盖范围扩大前(2016年3月1日至2018年2月28日)和扩大后(2018年3月1日至2019年9月30日)的产前筛查和诊断检测的使用情况及支出进行的真实世界比较。估计发病率比(IRR)及其95%置信区间(CI),以比较传统产前筛查方法和基于NIPT的产前筛查方法使用情况的变化。使用预算影响模型评估覆盖范围扩大后2020年的人均每月(PMPM)支出变化。
在覆盖范围扩大前和扩大后分别确定了5041例和4109例不同的妊娠。覆盖范围扩大前后孕妇的平均年龄±标准差一致(分别为30.35±3.35和30.33±3.28)。传统方法的筛查订单减少,扩大后时期的调整后IRR为扩大前时期的0.87倍(95%CI 0.85 - 0.90);NIPT的订单增加,扩大后时期的调整后IRR为扩大前时期的1.41倍(95%CI 1.32 - 1.51)。侵入性诊断检测在基线时较低(1.0%),覆盖范围扩大后没有变化。覆盖范围扩大后PMPM的变化估计为0.026美元。
为年龄小于35岁的女性扩大NIPT覆盖范围的PBRS协议与NIPT使用增加、传统筛查方法减少以及PMPM支出适度增加有关。