Samal Samir, Samir Shakti B, Patra Shantanu K, Rath Arun, Dash Abhilash, Nayak Biswajit, Mohanty Diganta
Department of Critical Care Medicine, IMS and SUM Hospital, Bhubaneswar, Odisha, India.
Indian J Crit Care Med. 2021 Feb;25(2):199-206. doi: 10.5005/jp-journals-10071-23720.
The objective of this review was to compare the effectiveness of Colistin monotherapy and combination therapy for the treatment of multidrug-resistant gram-negative bacterial infections.
PubMed, Cochrane Library.
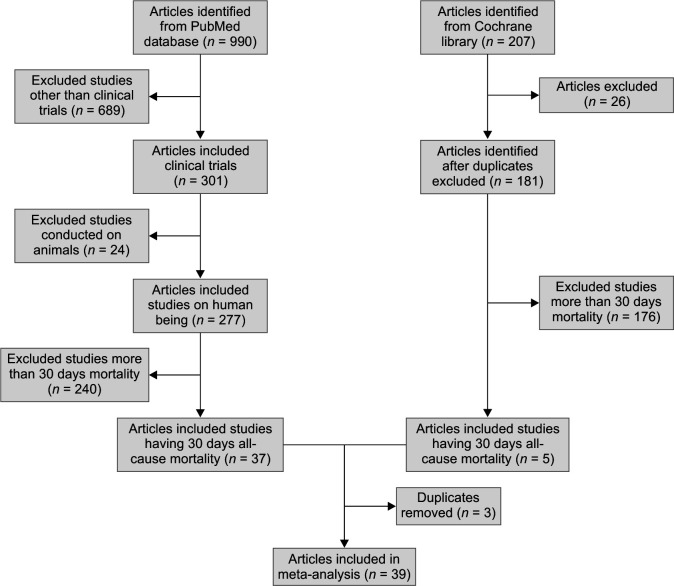
In this systematic review, we included all retrospective and prospective studies and randomized controlled trials (RCTs) that compared intravenous polymyxin monotherapy and combination therapy with any other antibiotic for treating multidrug-resistant infections. Studies using inhaled polymyxins with 5 or less than 5 patients were excluded. The primary outcome was 30-day all-cause mortality and if not reported at day 30 we extracted and documented the closest time point. Both crude outcome rates and adjusted effect estimates were extracted for mortality.
Search string used was "(Colistin OR polymyxin) AND ( OR OR OR OR ) AND (random OR prospective OR retrospective OR cohort OR observational OR blind)." Thirty-nine studies were included in our analysis; out of which 6 RCTs were included and 9 studies used carbapenem as the adjunctive antibiotic. Each study was screened and reviewed for eligibility independently by two authors and data extrapolated on an Excel sheet.
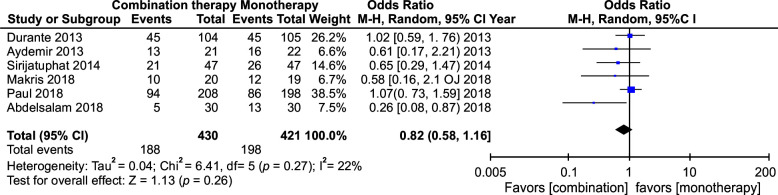
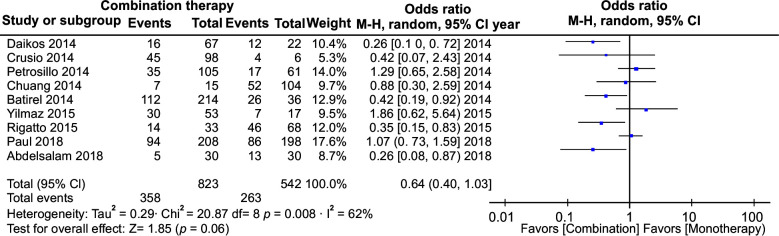
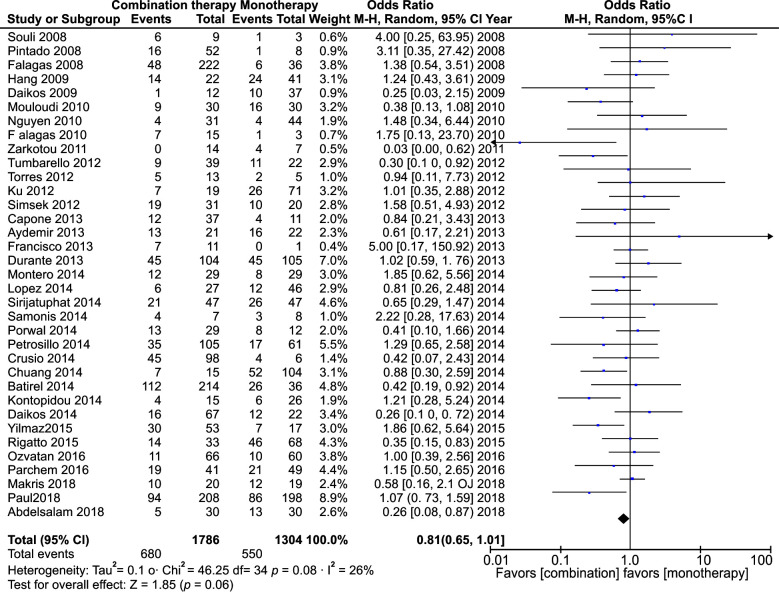
The meta-analysis of polymyxin monotherapy vs. combination therapy in multidrug-resistant infections yielded an odds ratio (OR) of 0.81 (95% confidence interval [CI]: 0.65-1.01) with minimal heterogeneity ( = 40%), whereas pooled analysis of this comparison in studies that included carbapenem as combination therapy yielded an OR of 0.64 (CI: 0.40-1.03; = 62%). Likewise, the pooled analysis of the RCTs yielded an OR of 0.82 (95% CI: 0.58-1.16, = 22%). All these showed no statistical significance. However, it was seen that polymyxin combination therapy was more effective in multidrug-resistant infections compared to polymyxin monotherapy. The effectiveness was more glaring when carbapenems were used as the combination drug instead of any other antibiotic and more so in many studies that used polymyxin combination therapy.
Although statistically insignificant, it would be prudent to use polymyxin combination therapy to treat multidrug-resistant gram-negative bacilli (GNB) infection over monotherapy with preference to use carbapenem as the adjunct alongside polymyxins.
Samal S, Mishra SB, Patra SK, Rath A, Dash A, Nayak B, et al. Polymyxin Monotherapy vs. Combination Therapy for the Treatment of Multidrug-resistant Infections: A Systematic Review and Meta-analysis. Indian J Crit Care Med 2021;25(2):199-206.
本综述的目的是比较多黏菌素单药治疗与联合治疗对多重耐药革兰氏阴性菌感染的疗效。
PubMed、Cochrane图书馆。
研究入选标准、干预措施及排除标准:在本系统评价中,我们纳入了所有比较静脉注射多黏菌素单药治疗及联合治疗与其他任何抗生素治疗多重耐药感染的回顾性和前瞻性研究以及随机对照试验(RCT)。使用吸入性多黏菌素且患者人数为5名或少于5名的研究被排除。主要结局为30天全因死亡率,若未在第30天报告,则提取并记录最接近的时间点。提取死亡率的粗结局率和校正效应估计值。
研究评估、数据提取与综合分析:使用的检索词为“(多黏菌素或黏菌素) AND (随机或前瞻性或回顾性或队列或观察性或盲法)”。我们的分析纳入了39项研究;其中包括6项RCT,9项研究使用碳青霉烯类作为辅助抗生素。由两位作者独立筛选和评估每项研究的入选资格,并将数据录入Excel表格。
多黏菌素单药治疗与联合治疗用于多重耐药感染的荟萃分析得出优势比(OR)为0.81(95%置信区间[CI]:0.65 - 1.01),异质性最小(I² = 40%),而在将碳青霉烯类作为联合治疗的研究中进行此比较的汇总分析得出OR为0.64(CI:0.40 - 1.03;I² = 62%)。同样,RCT的汇总分析得出OR为0.82(95%CI:0.58 - 1.16,I² = 22%)。所有这些均无统计学意义。然而,可以看出,与多黏菌素单药治疗相比,多黏菌素联合治疗在多重耐药感染中更有效。当使用碳青霉烯类而非其他任何抗生素作为联合用药时,这种有效性更为明显,在许多使用多黏菌素联合治疗的研究中更是如此。
尽管无统计学意义,但使用多黏菌素联合治疗而非单药治疗来处理多重耐药革兰氏阴性杆菌(GNB)感染可能更为审慎,且优先选择将碳青霉烯类作为多黏菌素的辅助用药。
Samal S, Mishra SB, Patra SK, Rath A, Dash A, Nayak B,等。多黏菌素单药治疗与联合治疗对多重耐药感染的疗效:一项系统评价和荟萃分析。《印度危重症医学杂志》2021;25(2):199 - 206。