Dutey-Magni Peter F, Williams Haydn, Jhass Arnoupe, Rait Greta, Lorencatto Fabiana, Hemingway Harry, Hayward Andrew, Shallcross Laura
Institute of Health Informatics, University College London, NW1 2DA, London, UK.
Four Seasons Health Care Group, SK9 1BU, Cheshire, UK.
Age Ageing. 2021 Jun 28;50(4):1019-1028. doi: 10.1093/ageing/afab060.
epidemiological data on COVID-19 infection in care homes are scarce. We analysed data from a large provider of long-term care for older people to investigate infection and mortality during the first wave of the pandemic.
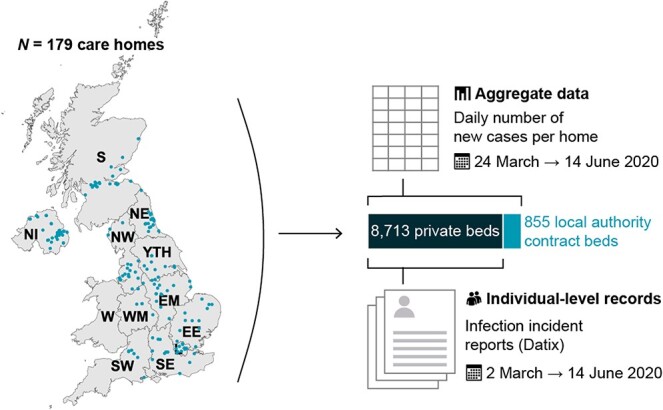
cohort study of 179 UK care homes with 9,339 residents and 11,604 staff. We used manager-reported daily tallies to estimate the incidence of suspected and confirmed infection and mortality in staff and residents. Individual-level electronic health records from 8,713 residents were used to model risk factors for confirmed infection, mortality and estimate attributable mortality.
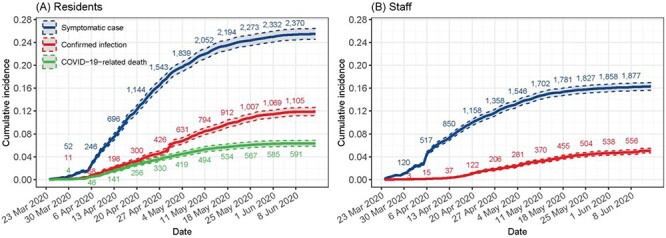
2,075/9,339 residents developed COVID-19 symptoms (22.2% [95% confidence interval: 21.4%; 23.1%]), while 951 residents (10.2% [9.6%; 10.8%]) and 585 staff (5.0% [4.7%; 5.5%]) had laboratory-confirmed infections. The incidence of confirmed infection was 152.6 [143.1; 162.6] and 62.3 [57.3; 67.5] per 100,000 person-days in residents and staff, respectively. Sixty-eight percent (121/179) of care homes had at least one COVID-19 infection or COVID-19-related death. Lower staffing ratios and higher occupancy rates were independent risk factors for infection.Out of 607 residents with confirmed infection, 217 died (case fatality rate: 35.7% [31.9%; 39.7%]). Mortality in residents with no direct evidence of infection was twofold higher in care homes with outbreaks versus those without (adjusted hazard ratio: 2.2 [1.8; 2.6]).
findings suggest many deaths occurred in people who were infected with COVID-19, but not tested. Higher occupancy and lower staffing levels were independently associated with risks of infection. Protecting staff and residents from infection requires regular testing for COVID-19 and fundamental changes to staffing and care home occupancy.
关于养老院中新冠病毒感染的流行病学数据匮乏。我们分析了一家大型老年人长期护理服务提供商的数据,以调查疫情第一波期间的感染情况和死亡率。
对英国179家养老院进行队列研究,这些养老院共有9339名居民和11604名工作人员。我们使用管理人员报告的每日统计数据来估计工作人员和居民中疑似和确诊感染及死亡的发生率。利用8713名居民的个人电子健康记录来建立确诊感染、死亡的风险因素模型,并估计可归因死亡率。
9339名居民中有2075人出现新冠症状(22.2%[95%置信区间:21.4%;23.1%]),而951名居民(10.2%[9.6%;10.8%])和585名工作人员(5.0%[4.7%;5.5%])有实验室确诊感染。居民和工作人员中确诊感染的发生率分别为每10万人日152.6[143.1;162.6]和62.3[57.3;67.5]。68%(121/179)的养老院至少有1例新冠感染或与新冠相关的死亡。较低的人员配备率和较高的入住率是感染的独立风险因素。在607名确诊感染的居民中,217人死亡(病死率:35.7%[31.9%;39.7%])。在有疫情爆发的养老院中,没有直接感染证据的居民的死亡率是没有爆发疫情的养老院中居民死亡率的两倍(调整后风险比:2.2[1.8;2.6])。
研究结果表明,许多死亡发生在感染了新冠病毒但未接受检测的人群中。较高的入住率和较低的人员配备水平与感染风险独立相关。保护工作人员和居民免受感染需要定期进行新冠病毒检测,并对人员配备和养老院入住率进行根本性改变。