Department of Visceral, Thoracic and Vascular Surgery, University Hospital and Faculty of Medicine Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany.
Department of General and Visceral Surgery, Friedrich Alexander University, Erlangen, Germany.
Langenbecks Arch Surg. 2021 Aug;406(5):1481-1489. doi: 10.1007/s00423-021-02138-4. Epub 2021 Mar 13.
The present study aimed to examine the impact of microscopically tumour-infiltrated resection margins (R1) in pancreatic ductal adenocarcinoma (PDAC) patients with advanced lymphonodular metastasis (pN1-pN2) on overall survival (OS).
This retrospective, multi-institutional analysis included patients undergoing surgical resection for PDAC at three tertiary university centres between 2005 and 2018. Subcohorts of patients with lymph node status pN0-N2 were stratified according to the histopathological resection status using Kaplan-Meier survival analysis.
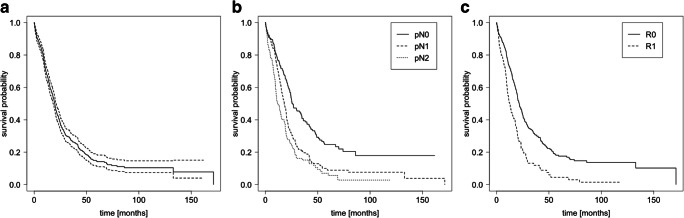
The OS of the entire cohort (n = 620) correlated inversely with the pN status (26 [pN0], 18 [pN1], 11.8 [pN2] months, P < 0.001) and R status (21.7 [R0], 12.5 [R1] months, P < 0.001). However, there was no statistically significant OS difference between R0 versus R1 in cases with advanced lymphonodular metastases: 19.6 months (95% CI: 17.4-20.9) versus 13.6 months (95% CI: 10.7-18.0) for pN1 stage and 13.7 months (95% CI: 10.7-18.9) versus 10.1 months (95% CI: 7.9-19.1) for pN2, respectively. Accordingly, N stage-dependent Cox regression analysis revealed that R status was a prognostic factor in pN0 cases only. Furthermore, there was no significant survival disadvantage for patients with R0 resection but circumferential resection margin invasion (≤ 1 mm; CRM+; 10.7 months) versus CRM-negative (13.7 months) cases in pN2 stages (P = 0.5).
An R1 resection is not associated with worse OS in pN2 cases. If there is evidence of advanced lymph node metastasis and a re-resection due to an R1 situation (e.g. at venous or arterial vessels) may substantially increase the perioperative risk, margin clearance in order to reach local control might be avoided with respect to the OS.
本研究旨在探讨在伴有淋巴结转移(pN1-pN2)的晚期胰腺导管腺癌(PDAC)患者中,显微镜下肿瘤浸润性切缘(R1)对总生存(OS)的影响。
本回顾性多中心分析纳入了 2005 年至 2018 年期间在三个三级大学中心接受 PDAC 手术切除的患者。使用 Kaplan-Meier 生存分析,根据淋巴结状态 pN0-N2 将患者亚组分为不同的组织病理学切除状态。
整个队列(n=620)的 OS 与 pN 状态呈负相关(26 [pN0]、18 [pN1]、11.8 [pN2] 个月,P<0.001)和 R 状态(21.7 [R0]、12.5 [R1] 个月,P<0.001)。然而,在伴有晚期淋巴结转移的情况下,R0 与 R1 之间的 OS 差异无统计学意义:pN1 期分别为 19.6 个月(95%CI:17.4-20.9)和 13.6 个月(95%CI:10.7-18.0),pN2 期分别为 13.7 个月(95%CI:10.7-18.9)和 10.1 个月(95%CI:7.9-19.1)。因此,N 分期的 Cox 回归分析显示,R 状态仅在 pN0 病例中是一个预后因素。此外,在 pN2 期,R0 切除但环周切缘受侵(≤1mm;CRM+;10.7 个月)与 CRM 阴性(13.7 个月)病例之间没有显著的生存劣势(P=0.5)。
在 pN2 病例中,R1 切除与 OS 无关。如果有证据表明存在淋巴结转移,并且由于 R1 情况(如静脉或动脉血管)而需要再次切除,这可能会显著增加围手术期风险,为了达到局部控制,可能会避免清除边缘,从而影响 OS。