Schenk Lorena M, Schneider Matthias, Bode Christian, Güresir Erdem, Junghanns Christoph, Müller Marcus, Putensen Christian, Vatter Hartmut, Zimmermann Julian, Schuss Patrick, Lehmann Felix
Department of Neurosurgery, University Hospital Bonn, Bonn, Germany.
Department of Anesthesiology and Critical Care Medicine, University Hospital Bonn, Bonn, Germany.
Front Neurol. 2021 Feb 25;12:636711. doi: 10.3389/fneur.2021.636711. eCollection 2021.
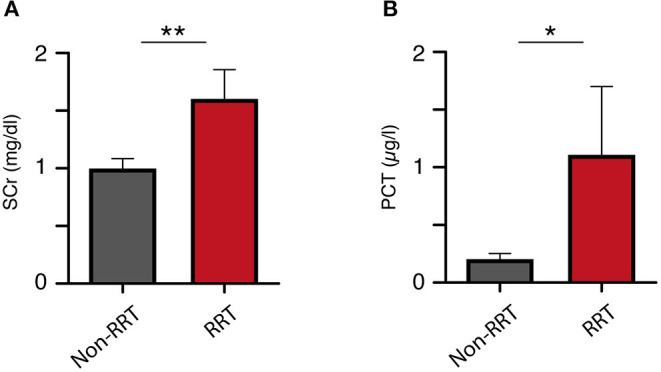
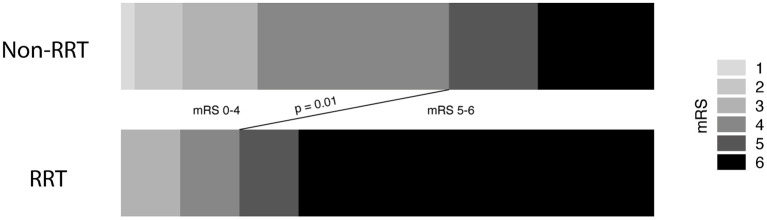
The need for continuous renal replacement therapy (CRRT) in patients with deep-seated intracerebral hemorrhage (ICH) requires sustained intensive care and often postpones further rehabilitation therapy. Therefore, an early identification of patients at risk is essential. From 2014 to 2019, all patients with deep-seated ICH who were admitted to intensive care for >3 days were included in the further analysis and retrospectively reviewed for the need for CRRT. All patients underwent CRRT with regional citrate anticoagulation for continuous veno-venous hemodialysis (CVVHD). Outcome was evaluated after 3 months using the modified Rankin scale. A multivariate analysis was performed to identify potential predictors for CRRT in patients with deep-seated ICH. After applying the inclusion criteria, a total of 87 patients with deep-seated spontaneous ICH were identified and further analyzed. During the first 48 h after admission, 21 of these patients developed early acute kidney injury (AKI; 24%). During treatment course, CRRT became necessary in nine patients suffering from deep-seated ICH (10%). The multivariate analysis revealed "development of AKI during the first 48 h" [ = 0.025, odds ratio (OR) 6.1, 95% confidence interval (CI) 1.3-29.8] and "admission procalcitonin (PCT) value >0.5 μg/l" ( = 0.02, OR 7.7, 95% CI 1.4-43.3) as independent and significant predictors for CRRT in patients with deep-seated ICH. Elevated serum levels of procalcitonin on admission as well as early development of acute renal injury are independent predictors of the need for renal replacement therapy in patients with deep-seated intracerebral bleeding. Therefore, further research is warranted to identify these vulnerable patients as early as possible to enable adequate treatment.
深部脑出血(ICH)患者对持续肾脏替代治疗(CRRT)的需求需要持续的重症监护,并且常常会推迟进一步的康复治疗。因此,早期识别有风险的患者至关重要。2014年至2019年,所有因深部ICH入住重症监护病房超过3天的患者被纳入进一步分析,并对CRRT需求进行回顾性评估。所有患者均接受了采用局部枸橼酸抗凝的持续静脉-静脉血液透析(CVVHD)的CRRT治疗。3个月后使用改良Rankin量表评估预后。进行多因素分析以确定深部ICH患者CRRT的潜在预测因素。应用纳入标准后,共识别出87例深部自发性ICH患者并进行进一步分析。入院后的最初48小时内,其中21例患者发生早期急性肾损伤(AKI;24%)。在治疗过程中,9例深部ICH患者需要进行CRRT(10%)。多因素分析显示,“入院后最初48小时内发生AKI”[P = 0.025,比值比(OR)6.1,95%置信区间(CI)1.3 - 29.8]和“入院时降钙素原(PCT)值>0.5μg/L”(P = 0.02,OR 7.7,95% CI 1.4 - 43.3)是深部ICH患者CRRT的独立且显著的预测因素。入院时降钙素原血清水平升高以及急性肾损伤的早期发生是深部脑出血患者肾脏替代治疗需求的独立预测因素。因此,有必要进行进一步研究以尽早识别这些易损患者,以便进行适当治疗。