Power Alexandra D, Merritt Robert E, Abdel-Rasoul Mahmoud, Moffatt-Bruce Susan D, D'Souza Desmond M, Kneuertz Peter J
Division of Thoracic Surgery, Department of Surgery, The Ohio State University Wexner Medical Center, Columbus, OH, USA.
Center for Biostatistics, The Ohio State University College of Medicine, Columbus, OH, USA.
J Thorac Dis. 2021 Feb;13(2):812-823. doi: 10.21037/jtd-20-2950.
Understanding the risk of conversion from video-assisted thoracic surgery (VATS) to thoracotomy is important when considering patient selection and preoperative surgical risk assessment. This review aims to estimate the rate of intraoperative conversions to thoracotomy, predictive factors, and associated outcomes for VATS anatomic lung resections.
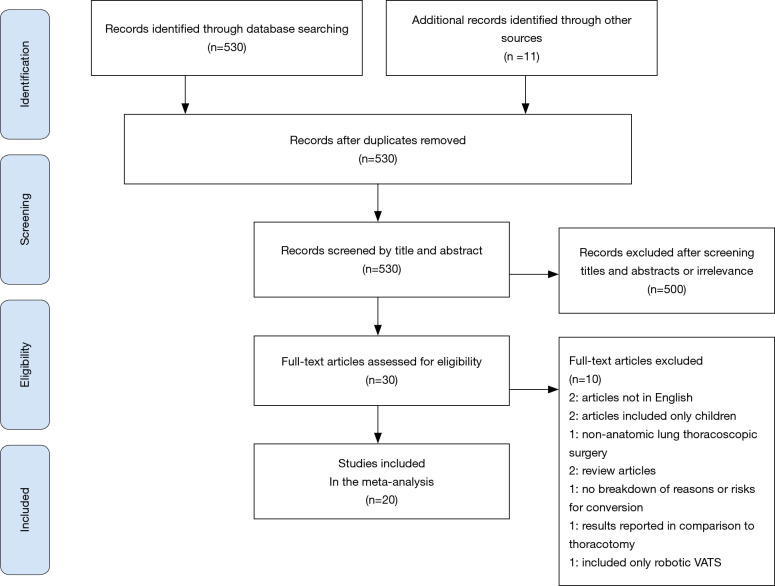
PubMed/MEDLINE and EMBASE were searched systematically in May of 2020. Observational studies examining conversions of VATS anatomic resections to thoracotomy were included. Conversion rates, causes, risk factors, and post-operative outcomes were reviewed and analyzed in aggregate.
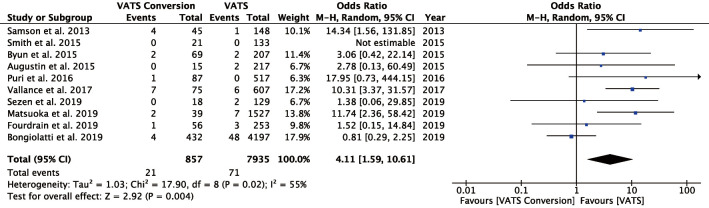
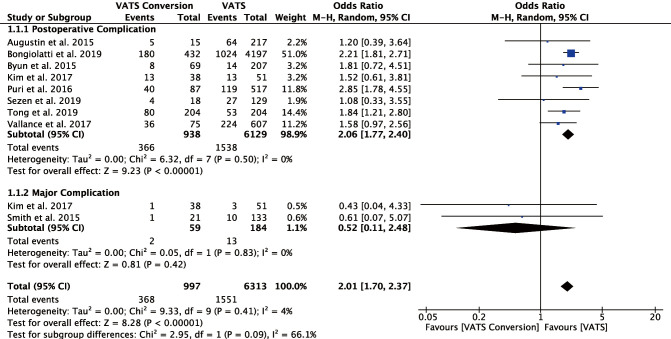
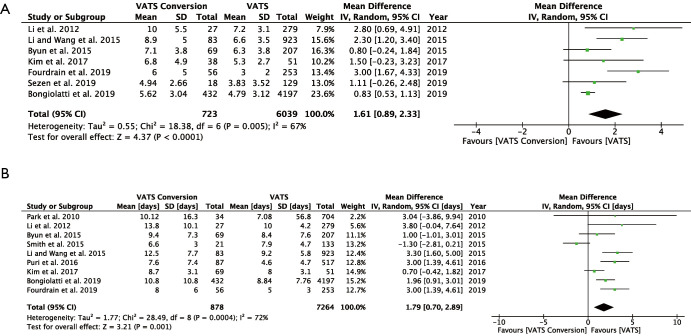
Twenty retrospective studies were reviewed, with a total of 72,932 patients undergoing VATS anatomic lung resection. The median conversion rate was 9.6% (95% CI: 6.6-13.9%). Nine studies reported a total of 114 emergency conversions, with a median incidence rate of 1.3% (95% CI: 0.6-2.8%). The most common reasons for thoracotomy were vascular injury/bleeding, difficulty lymph node dissection, and adhesions, accounting for 27.9%, 26.2% and 19% of conversions, respectively. Risk factors for conversion varied, but frequently included nodal disease, large tumors, and induction therapy. The risk of complications (OR 2.06; 95% CI: 1.77-2.40) and mortality (OR 4.11; 95% CI: 1.59-10.61) were significantly increased following conversions. There was also a significant increase in chest tube duration and length of stay following conversion.
The risk of conversion to thoracotomy may be as high as one in ten patients undergoing VATS anatomic lung resections, but may vary significantly based on patient selection. Although emergent conversions are rare, the need for thoracotomy may significantly increase postoperative morbidity and mortality.
在考虑患者选择和术前手术风险评估时,了解电视辅助胸腔镜手术(VATS)转为开胸手术的风险很重要。本综述旨在评估VATS解剖性肺切除术中转为开胸手术的发生率、预测因素及相关结局。
于2020年5月系统检索了PubMed/MEDLINE和EMBASE。纳入了观察VATS解剖性切除转为开胸手术的研究。对转化率、原因、危险因素及术后结局进行汇总回顾和分析。
共纳入20项回顾性研究,总计72932例患者接受了VATS解剖性肺切除。中位转化率为9.6%(95%CI:6.6 - 13.9%)。9项研究共报告了114例急诊转为开胸手术,中位发生率为1.3%(95%CI:0.6 - 2.8%)。开胸手术最常见的原因是血管损伤/出血、淋巴结清扫困难和粘连,分别占转为开胸手术的27.9%、26.2%和19%。转为开胸手术的危险因素各不相同,但常见的有淋巴结疾病、肿瘤体积大及诱导治疗。转为开胸手术后并发症风险(OR 2.06;95%CI:1.77 - 2.40)和死亡率(OR 4.11;95%CI:1.59 - 10.61)显著增加。转为开胸手术后胸腔引流管留置时间和住院时间也显著延长。
接受VATS解剖性肺切除的患者中,转为开胸手术的风险可能高达十分之一,但会因患者选择的不同而有显著差异。虽然急诊转为开胸手术很少见,但转为开胸手术可能会显著增加术后发病率和死亡率。