Wang Jing, Zhang Baozhong, Pang Qingsong, Zhang Tian, Chen Xi, Er Puchun, Wang Yuwen, You Jinqiang, Wang Ping
Department of Radiation Oncology, Tianjin Medical University Cancer Institute and Hospital, Key Laboratory of Cancer Prevention and Therapy, National Clinical Research Center for Cancer, Tianjin's Clinical Research Centre for Cancer, Tianjin, China.
J Thorac Dis. 2021 Feb;13(2):883-892. doi: 10.21037/jtd-20-1587.
To establish a nomogram for predicting the outcome of EGFR-mutated lung adenocarcinoma patients with brain metastases (BMs) and to estimate the efficacy of different therapeutic strategies.
The data of 129 cases with BM from the period between January 1st 2011 and December 31st 2014 were collected, and all of the cases were pathologically confirmed to be lung adenocarcinoma, stages I-IV and with 19 and/or 21 exon mutations of EGFR. Cox regression analysis and log-rank test were used for data analysis. The nomogram was used to establish the progression models.
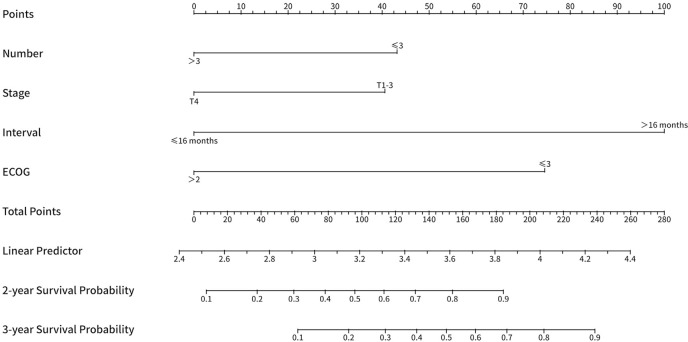
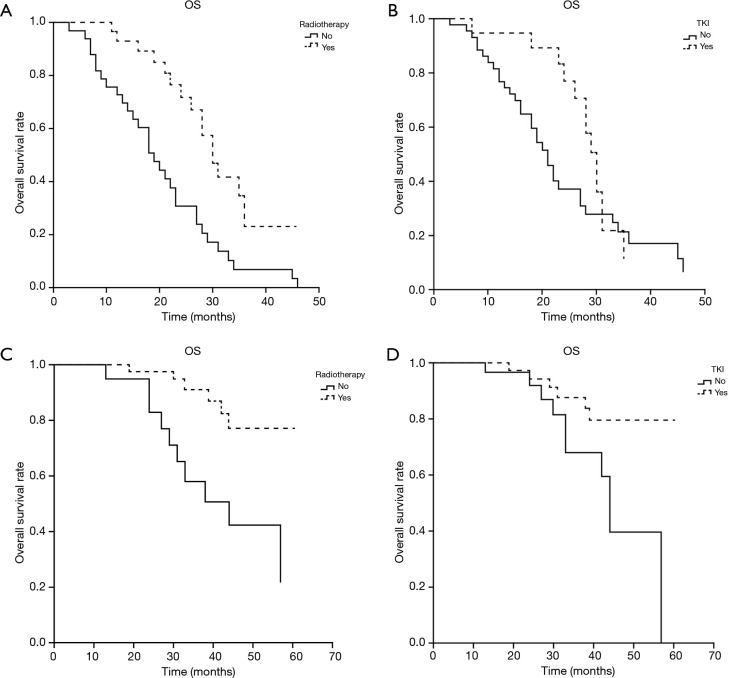
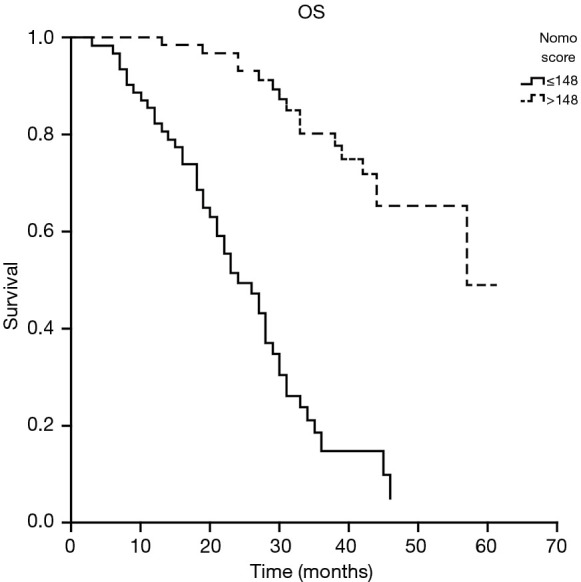
In the univariate analysis, the stage, ECOG score, interval between the diagnosis of lung cancer and BM, the number of brain metastatic lesions, and the diameter of the maximal brain metastatic lesion correlated well with overall survival (OS). In multivariate Cox proportional hazard analysis, the ECOG score, interval between the diagnosis of lung cancer and BM, and the number of brain metastatic lesions correlated well with the OS. Patients were divided into the poor prognostic group and the good prognostic group based on the nomogram prognostic model score. Subgroup analysis showed that in the poor prognostic group, the OS of patients who received radiotherapy was better than that of the patients who did not receive radiotherapy as the first-line treatment (30 19 months, P<0.05). The OS was 30 months in the TKI subgroup and 21 months in the no TKI subgroup, but no statistical difference was found (P>0.05). Patients in the good prognostic group who received radiotherapy had a better 3-y OS rate than the patients who received no radiotherapy as the first-line treatment (91.2% 58.1%, P<0.05). The 3-y OS rate was 87.6% in the TKI subgroup and 67.8% in the no TKI group (P<0.05).
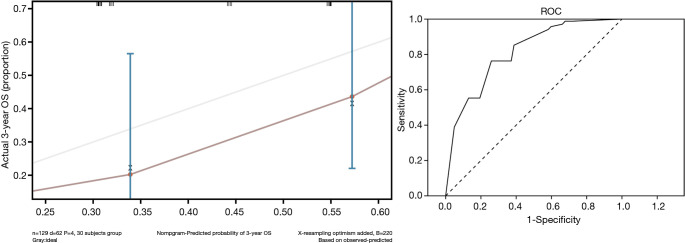
We established an effective nomogram model to predict the progression of EGFR-mutated lung adenocarcinoma patients with BM and the therapeutic effect of the individual treatments. Radiotherapy was beneficial for the patients of both the poor and good prognostic groups, but TKI may be better suited for treating the patients with good prognosis.
建立一种列线图,用于预测表皮生长因子受体(EGFR)突变的肺腺癌脑转移(BM)患者的预后,并评估不同治疗策略的疗效。
收集2011年1月1日至2014年12月31日期间129例BM患者的数据,所有病例经病理确诊为肺腺癌,分期为I-IV期,且存在EGFR第19和/或21外显子突变。采用Cox回归分析和对数秩检验进行数据分析。使用列线图建立进展模型。
单因素分析中,分期、美国东部肿瘤协作组(ECOG)评分、肺癌诊断与BM的间隔时间、脑转移瘤数量及最大脑转移瘤直径与总生存期(OS)密切相关。多因素Cox比例风险分析中,ECOG评分、肺癌诊断与BM的间隔时间及脑转移瘤数量与OS密切相关。根据列线图预后模型评分将患者分为预后不良组和预后良好组。亚组分析显示,在预后不良组中,接受放疗患者的OS优于未接受放疗作为一线治疗的患者(30对19个月,P<0.05)。TKI亚组的OS为30个月,非TKI亚组为21个月,但差异无统计学意义(P>0.05)。预后良好组中接受放疗的患者3年OS率优于未接受放疗作为一线治疗的患者(91.2%对58.1%,P<0.05)。TKI亚组的3年OS率为87.6%,非TKI组为67.8%(P<0.05)。
我们建立了一种有效的列线图模型,用于预测EGFR突变的肺腺癌BM患者的病情进展及个体化治疗的疗效。放疗对预后不良组和预后良好组患者均有益,但TKI可能更适合治疗预后良好的患者。