Basham C Andrew, Karim Mohammad E, Cook Victoria J, Patrick David M, Johnston James C
School of Population and Public Health, University of British Columbia, Vancouver, Canada.
British Columbia Centre for Disease Control, Vancouver, Canada.
EClinicalMedicine. 2021 Feb 26;33:100752. doi: 10.1016/j.eclinm.2021.100752. eCollection 2021 Mar.
Current epidemiological evidence of post-TB airway disease is largely cross-sectional and derived from high-TB-incidence settings. We present the first cohort study of post-TB airway disease in a low-TB-incidence setting.
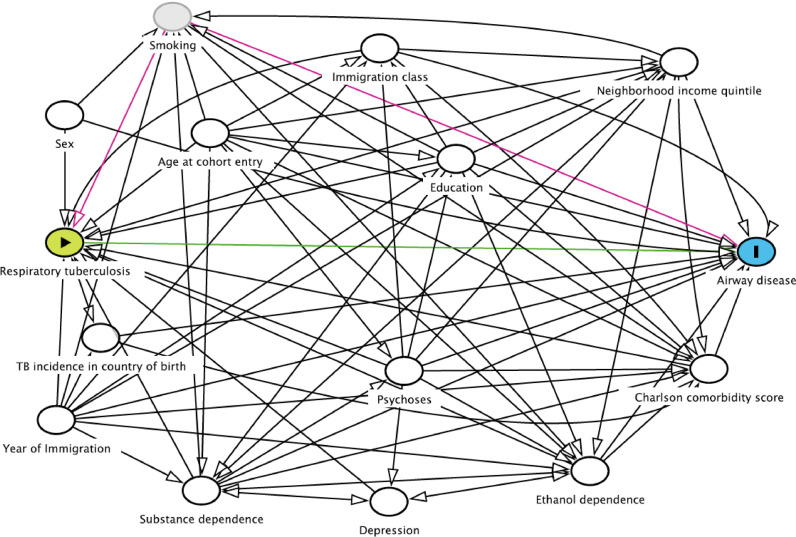
(1) analyze the risk of airway disease by respiratory TB, (2) assess potential unmeasured confounding between TB and airway disease, and (3) investigate TB effect measure modification.
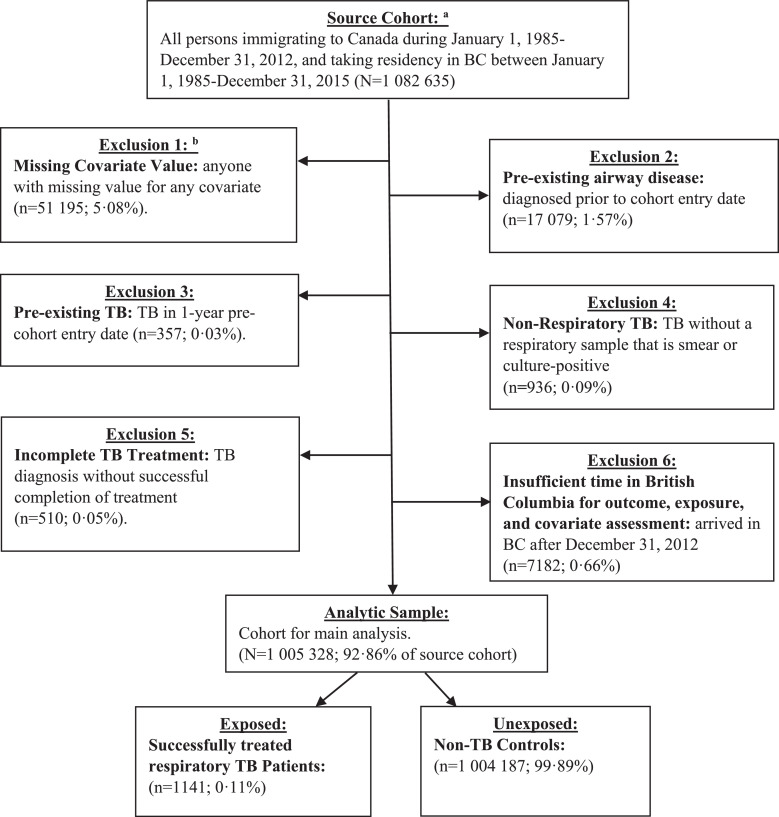
A population-based cohort study using healthcare claims data for immigrants to British Columbia (BC), Canada, 1985-2015. Airway disease included chronic airway obstruction, asthma, bronchitis, bronchiolitis, and emphysema. Respiratory TB was defined from TB registry data. Cox proportional hazards (PH) regressions were used to analyze time-to-airway disease by respiratory TB. Sensitivity analyses included varying definitions of TB and airway disease. Potential unmeasured confounding by smoking was evaluated by E-value and hybrid least absolute shrinkage and selection operator (LASSO)-high-dimensional propensity score (hdPS).
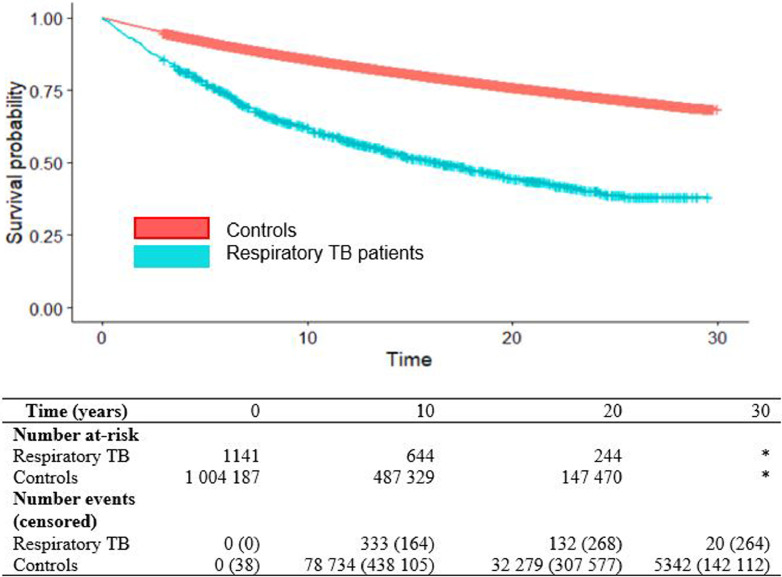
In our cohort ( = 1 005 328; n=1141) there were 116 840 incident cases of airway disease during our 30-year study period (10.43 per 1,000 person-years of follow-up), with cumulative incidence of 42·5% among respiratory TB patients compared with 11·6% among non-TB controls. The covariate-adjusted hazard ratio (aHR) for airway disease by respiratory TB was 2·08 (95% CI: 1·91-2·28) with E-value=3·58. The LASSO-hdPS analysis produced aHR=2·26 (95% CI: 2·07-2·47).
A twofold higher risk of airway disease was observed among immigrants diagnosed with respiratory TB, compared with non-TB controls, in a low-TB-incidence setting. Unmeasured confounding is unlikely to explain this relationship. Models of post-TB care are needed.
Canadian Institutes of Health Research.
目前关于结核病后气道疾病的流行病学证据大多是横断面研究,且来自结核病高发病率地区。我们开展了首例在结核病低发病率地区针对结核病后气道疾病的队列研究。
(1)分析呼吸道结核病引发气道疾病的风险;(2)评估结核病与气道疾病之间潜在的未测量混杂因素;(3)研究结核病效应测量修正。
一项基于人群的队列研究,使用了1985 - 2015年加拿大不列颠哥伦比亚省(BC)移民的医疗保健索赔数据。气道疾病包括慢性气道阻塞、哮喘、支气管炎、细支气管炎和肺气肿。呼吸道结核病由结核病登记数据定义。采用Cox比例风险(PH)回归分析呼吸道结核病引发气道疾病的时间。敏感性分析包括对结核病和气道疾病的不同定义。通过E值以及混合最小绝对收缩和选择算子(LASSO)-高维倾向评分(hdPS)评估吸烟可能导致的未测量混杂因素。
在我们的队列中(n = 1 005 328;n = 1141),在30年的研究期间有116 840例气道疾病发病病例(每1000人年随访中有10.43例),呼吸道结核病患者的累积发病率为42.5%,而非结核病对照组为11.6%。经协变量调整后,呼吸道结核病引发气道疾病的风险比(aHR)为2.08(95%置信区间:1.91 - 2.28),E值为3.58。LASSO - hdPS分析得出aHR = 2.26(95%置信区间:2.07 - 2.47)。
在结核病低发病率地区,与非结核病对照组相比,被诊断为呼吸道结核病的移民患气道疾病的风险高出两倍。未测量的混杂因素不太可能解释这种关系。需要建立结核病后护理模式。
加拿大卫生研究院。