Department of Medicine, 12222UCLA-Olive View Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA.
Division of Pulmonary and Critical Care Medicine, Ronald Reagan 12222UCLA Medical Center, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA.
J Intensive Care Med. 2021 Jun;36(6):646-654. doi: 10.1177/0885066621989959. Epub 2021 Mar 15.
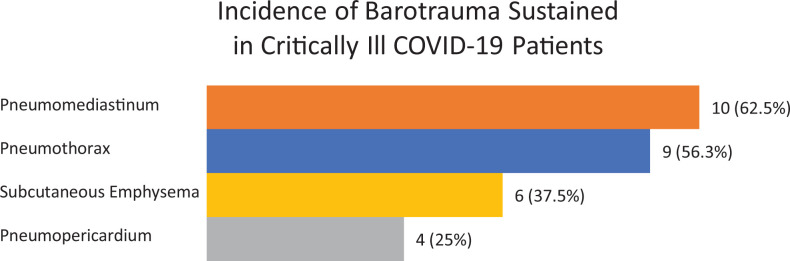
OBJECTIVE.: To report the high incidence of barotrauma in critically ill patients admitted to the intensive care unit (ICU) with coronavirus disease 2019 (COVID-19) and to discuss its implications.
DESIGN.: Retrospective cohort study.
SETTING.: ICU of an academic county hospital in Los Angeles, CA admitted from March 15-June 20, 2020.
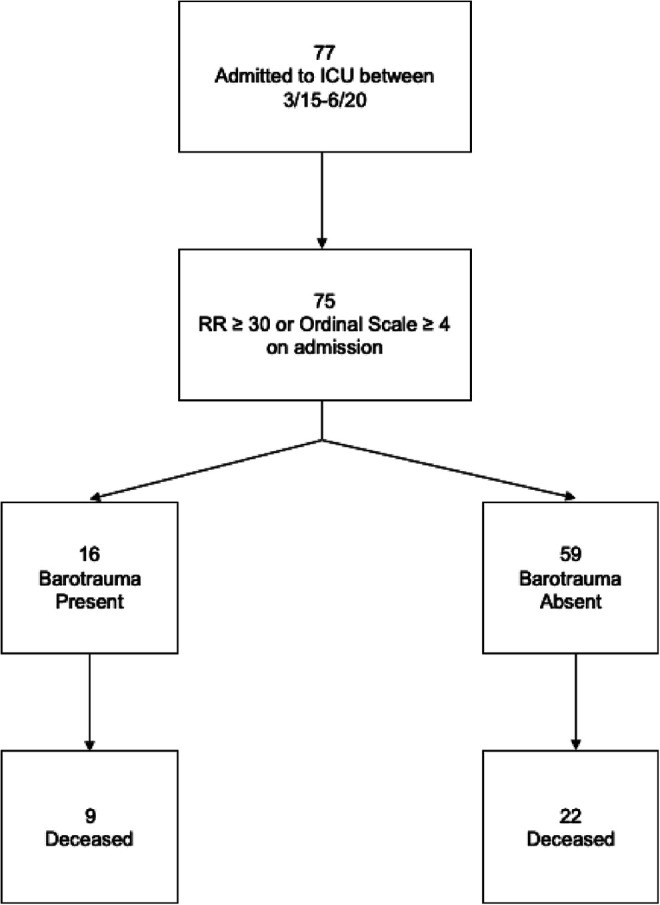
PATIENTS.: 77 patients with COVID-19 pneumonia. 75 patients met inclusion criteria.
RESULTS.: 21% of patients with severe COVID-19 sustained barotrauma (33% of patients receiving IMV, 8% of patients receiving (NIV). There were no differences between the barotrauma and non-barotrauma groups regarding demographics, illness severity, or medications received, nor tidal volume or average/peak airway pressures in those receiving IMV. In the barotrauma group there was a greater proportion of patients receiving therapeutic anticoagulation (81% vs. 47%, p = 0.023) and ventilated using airway pressure release ventilation mode (13% vs. 0%, p = 0.043). Barotrauma was associated with increased likelihood of receiving a tracheostomy (OR 2.58 [0.23-4.9], p = 0.018]), longer median ICU length of stay (17 days vs. 7 days, p = 0.03), and longer median length of hospitalization (26 days vs. 14 days, p < 0.001). There was also a trend toward prolonged median duration of IMV (12.5 days vs 7 days, p = 0.13) and higher average mortality (56% vs 37%, p = 0.25).
CONCLUSIONS.: Barotrauma is seen in 5-12% of patients with ARDS receiving IMV and is exceedingly rare in patients receiving NIV. We report a high incidence of barotrauma observed in critically ill patients with COVID-19 requiring either NIV or IMV. While there was a trend toward increased mortality in patients with barotrauma, this did not reach statistical significance. The increased incidence of barotrauma with COVID-19 may be a product of the pathophysiology of this disease state and a heightened inflammatory response causing rampant acute lung injury. Evidence-based medicine and lung-protective ventilation should remain the mainstay of treatment.
报告新冠肺炎(COVID-19)重症患者入住重症监护病房(ICU)时气压伤的高发率,并讨论其影响。
回顾性队列研究。
加利福尼亚州洛杉矶一家学术县医院的 ICU,于 2020 年 3 月 15 日至 6 月 20 日收治。
77 例 COVID-19 肺炎患者。75 例符合纳入标准。
21%的严重 COVID-19 患者发生气压伤(接受有创机械通气的患者中为 33%,接受无创通气的患者中为 8%)。气压伤组和非气压伤组在人口统计学、疾病严重程度或接受的药物、接受有创机械通气的患者的潮气量或平均/峰值气道压力方面无差异。气压伤组接受治疗性抗凝的患者比例较高(81%比 47%,p=0.023),使用气道压力释放通气模式通气的患者比例较高(13%比 0%,p=0.043)。气压伤与气管切开术(OR 2.58[0.23-4.9],p=0.018)、ICU 中位住院时间延长(17 天比 7 天,p=0.03)和中位住院时间延长(26 天比 14 天,p<0.001)的可能性增加有关。有创机械通气的中位持续时间延长(12.5 天比 7 天,p=0.13)和平均死亡率升高(56%比 37%,p=0.25)也呈趋势。
接受有创机械通气的 ARDS 患者中气压伤发生率为 5-12%,接受无创通气的患者中气压伤发生率极低。我们报告了 COVID-19 重症患者中气压伤发生率较高,这些患者需要接受无创通气或有创机械通气。虽然气压伤患者的死亡率有升高趋势,但未达到统计学意义。COVID-19 气压伤发生率增加可能是该疾病状态的病理生理学和弥漫性急性肺损伤引起的炎症反应增强的结果。循证医学和肺保护性通气应仍然是治疗的主要方法。