Department of Advanced Medical and Surgical Sciences, MRI Research Center Vanvitelli-FISM, University of Campania "Luigi Vanvitelli", Piazza Miraglia 2, 80138, Naples, Italy.
Department of Psychology, University of Campania "Luigi Vanvitelli", Viale Ellittico 31, 81100, Caserta, Italy.
J Neurol. 2021 Sep;268(9):3444-3455. doi: 10.1007/s00415-021-10519-4. Epub 2021 Mar 15.
Subjective complaints of cognitive deficits are not necessarily consistent with objective evidence of cognitive impairment in Parkinson's disease (PD). Here we examined the factors associated with the objective-subjective cognitive discrepancy.
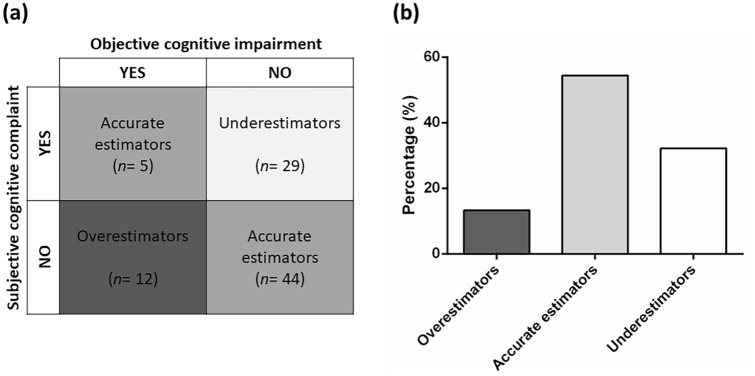
We consecutively enrolled 90 non-demented patients with PD who completed the Parkinson's Disease Cognitive Functional Rating Scale (subjective cognitive measure) and the Montreal Cognitive Assessment (MoCA; objective cognitive measure). The patients were classified as "Overestimators", "Accurate estimators", and "Underestimators" on the basis of the discrepancy between the objective vs. subjective cognitive measures. To identify the factors distinguishing these groups from each other, we used chi-square tests or one-way analyses of variance, completed by logistic and linear regression analyses.
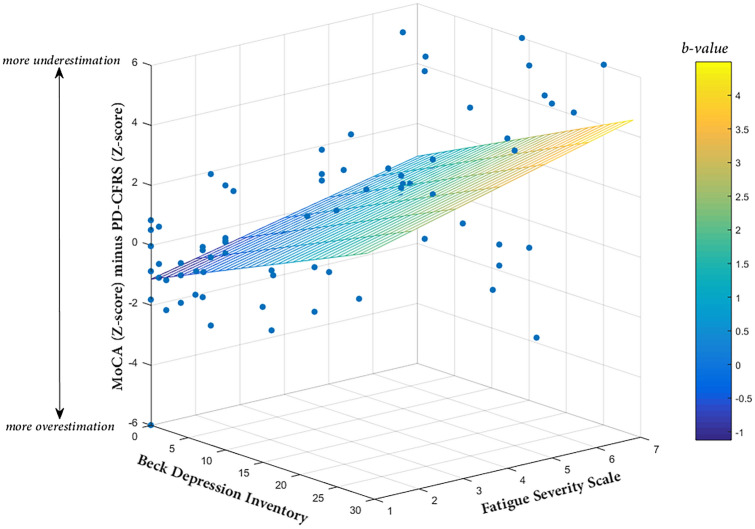
Forty-nine patients (54.45%) were classified as "Accurate estimators", 29 (32.22%) as "Underestimators", and 12 (13.33%) as "Overestimators". Relative to the other groups, the "Underestimators" scored higher on the Fatigue Severity Scale (FSS), Beck Depression Inventory (BDI), and Parkinson Anxiety Scale (p < 0.01). Logistic regression confirmed that FSS and BDI scores distinguished the "Underestimators" group from the others (p < 0.05). Linear regression analyses also indicated that FSS and BDI scores positively related to objective-subjective cognitive discrepancy (p < 0.01). "Overestimators" scored lower than other groups on the MoCA's total score and attention and working memory subscores (p < 0.01).
In more than 45% of consecutive non-demented patients with PD, we found a 'mismatch' between objective and subjective measures of cognitive functioning. Such discrepancy, which was related to the presence of fatigue and depressive symptoms and frontal executive impairments, should be carefully evaluated in clinical setting.
帕金森病(PD)患者的主观认知缺陷主诉不一定与客观认知损害的证据一致。在此,我们研究了与客观-主观认知差异相关的因素。
我们连续纳入 90 例非痴呆 PD 患者,他们完成了帕金森病认知功能评定量表(主观认知测量)和蒙特利尔认知评估(MoCA;客观认知测量)。根据客观与主观认知测量之间的差异,将患者分为“高估者”、“准确估计者”和“低估者”。为了确定这些组彼此之间的区别因素,我们使用卡方检验或单向方差分析,完成逻辑回归和线性回归分析。
49 例患者(54.45%)被归类为“准确估计者”,29 例(32.22%)为“低估者”,12 例(13.33%)为“高估者”。与其他组相比,“低估者”在疲劳严重程度量表(FSS)、贝克抑郁量表(BDI)和帕金森焦虑量表(p < 0.01)上的评分更高。逻辑回归证实 FSS 和 BDI 评分可区分“低估者”组与其他组(p < 0.05)。线性回归分析也表明 FSS 和 BDI 评分与客观-主观认知差异呈正相关(p < 0.01)。“高估者”在 MoCA 的总分和注意力及工作记忆子项上的得分低于其他组(p < 0.01)。
在超过 45%的连续非痴呆 PD 患者中,我们发现客观和主观认知功能测量之间存在“不匹配”。这种差异与疲劳和抑郁症状以及额叶执行功能障碍有关,在临床环境中应仔细评估。