Department of Rheumatology, Erasmus Medical Center.
Department of Rheumatology, Maasstad Hospital.
Rheumatology (Oxford). 2021 Dec 1;60(12):5765-5774. doi: 10.1093/rheumatology/keab251.
To evaluate the 1-year cost-effectiveness between three different initial treatment strategies in autoantibody-negative RA patients, according to 2010 criteria.
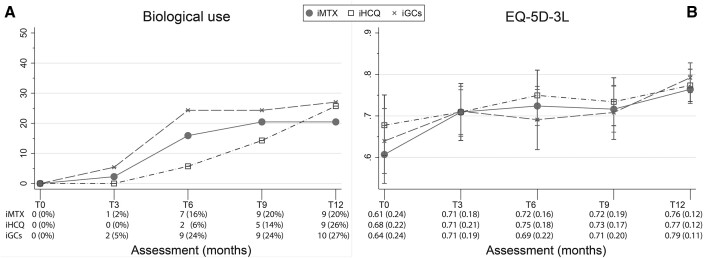
For this analysis we selected all RA patients within the intermediate probability stratum of the treatment in the Rotterdam Early Arthritis Cohort (tREACH) trial. The tREACH had a treat-to-target approach, aiming for low DAS <2.4, and treatment adjustments could occur every 3 months. Initial treatment strategies consisted of MTX 25 mg/week (initial MTX, iMTX), iHCQ 400 mg/day or an oral glucocorticoids tapering scheme without DMARDs (iGCs). Data on quality-adjusted life-years, measured with the European Quality of Life 5-Dimensions 3 Levels (EQ-5D-3L), healthcare and productivity costs were used.
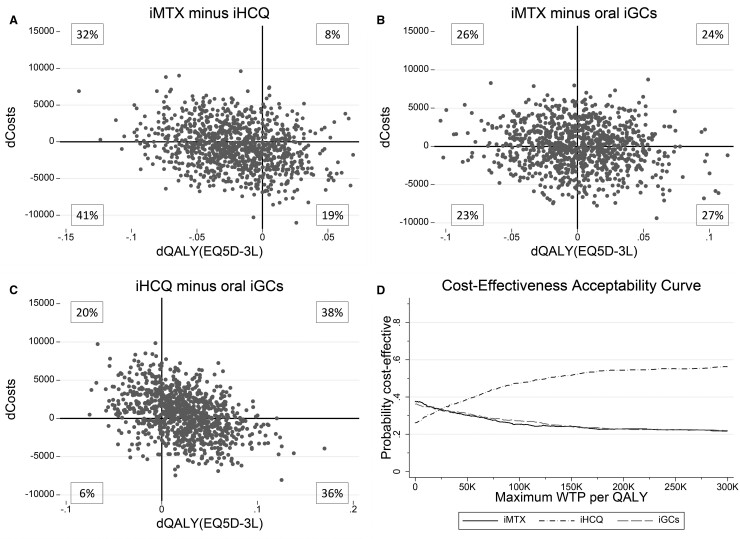
Average quality-adjusted life-years (s.d.), for iMTX, iHCQ and iGCs were respectively 0.71 (0.14), 0.73 (0.14) and 0.71 (0.15). The average total costs (s.d.) for iMTX, iHCQ and iGCs were, respectively, €10 832 (14.763), €11 208 (12.801) and €10 502 (11.973). Healthcare costs were mainly determined by biological costs, which were significantly lower in the iHCQ group compared with iGCs (P < 0.05). However, costs due to presenteeism were the highest in the iHCQ group (55%) followed by iMTX (27%) and iGCs (18%). The incremental cost-effectiveness ratios did not differ between treatment strategies. At a willingness-to-pay level of €50 000, the Dutch threshold for reimbursement of medical care, iHCQ had the highest probability (38.7%) of being cost-effective, followed by iGCs (31.1%) and iMTX (30.2%).
iHCQ had the lowest healthcare and highest productivity costs, resulting in a non-significant incremental cost-effectiveness ratio. However, iHCQ had the highest chance of being cost-effective at the Dutch willingness-to-pay threshold for healthcare reimbursement. Therefore, we believe that iHCQ is a good alternative to iMTX in autoantibody-negative RA patients, but validation is needed.
ISRCTN26791028.
根据 2010 年标准,评估三种不同初始治疗策略在抗核抗体阴性 RA 患者中的 1 年成本效益。
本分析选取了 Rotterdam Early Arthritis Cohort(tREACH)试验中治疗处于中概率分层的所有 RA 患者。tREACH 采用了达标治疗方法,目标是 DAS<2.4,并每 3 个月进行一次治疗调整。初始治疗策略包括每周 25mg MTX(初始 MTX,iMTX)、每天 400mg HCQ 或不使用 DMARD 的口服糖皮质激素递减方案(iGCs)。使用欧洲生活质量 5 维 3 水平(EQ-5D-3L)测量的质量调整生命年和医疗保健及生产力成本数据。
iMTX、iHCQ 和 iGCs 的平均质量调整生命年(标准差)分别为 0.71(0.14)、0.73(0.14)和 0.71(0.15)。iMTX、iHCQ 和 iGCs 的平均总费用(标准差)分别为 10832 欧元(14.763 欧元)、11208 欧元(12.801 欧元)和 10502 欧元(11.973 欧元)。医疗保健费用主要由生物成本决定,iHCQ 组的生物成本明显低于 iGCs 组(P<0.05)。然而,由于旷工导致的成本在 iHCQ 组最高(55%),其次是 iMTX 组(27%)和 iGCs 组(18%)。增量成本效益比在治疗策略之间没有差异。在愿意支付 50000 欧元的水平下,荷兰医疗保健报销的阈值,iHCQ 具有最高的成本效益概率(38.7%),其次是 iGCs(31.1%)和 iMTX(30.2%)。
iHCQ 的医疗保健成本最低,生产力成本最高,导致增量成本效益比不显著。然而,在荷兰医疗保健报销的意愿支付阈值下,iHCQ 具有最高的成本效益概率。因此,我们认为 iHCQ 是抗核抗体阴性 RA 患者的 iMTX 的一个较好的替代方案,但需要验证。
ISRCTN26791028。