Weerasinghe Swarna S, Campbell Sam G
Department of Community Health and Epidemiology, Dalhousie University, Halifax, CAN.
Department of Emergency Medicine, Dalhousie University, Halifax, CAN.
Cureus. 2021 Feb 8;13(2):e13225. doi: 10.7759/cureus.13225.
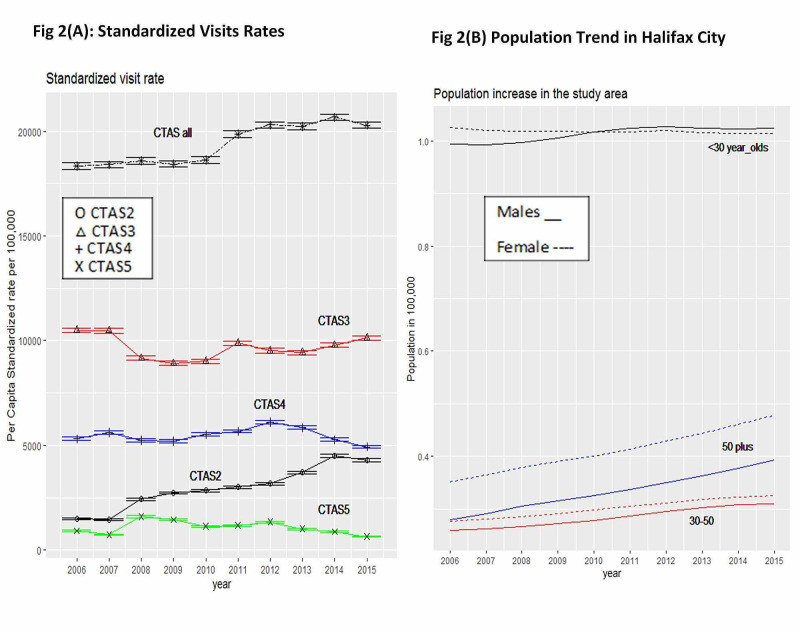
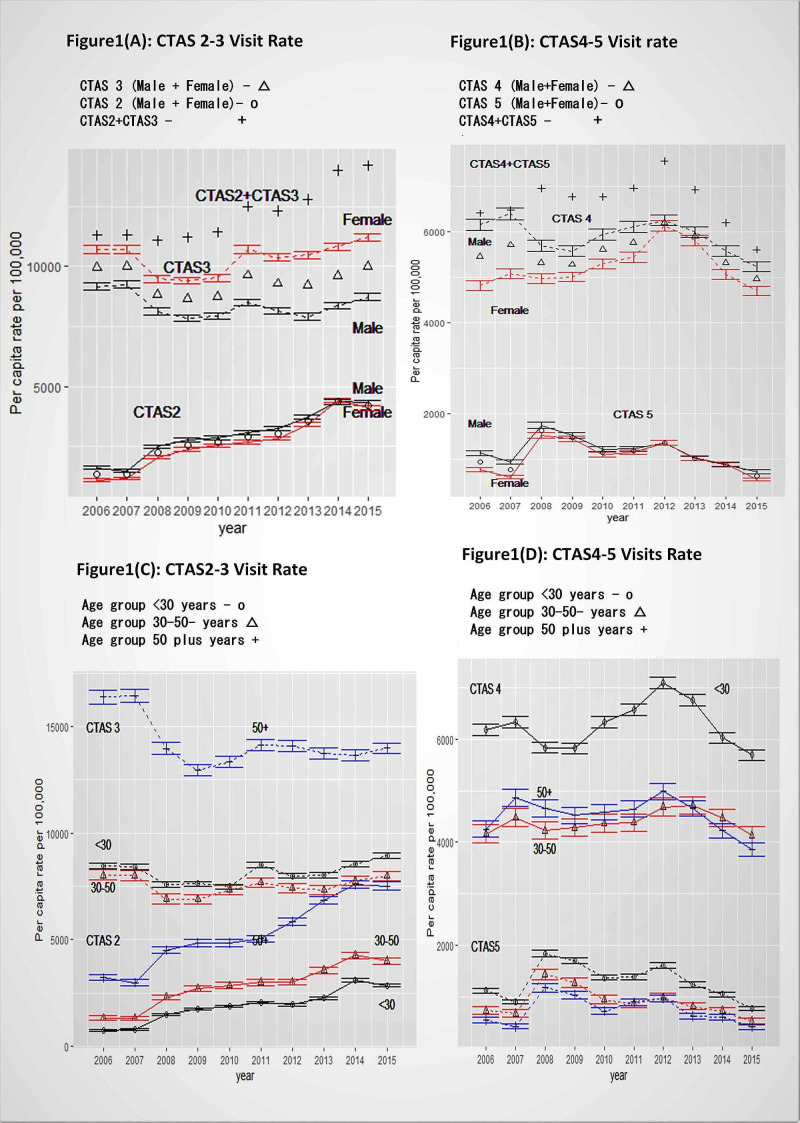
Introduction Canadian emergency departments (EDs) are struggling under the weight of increased use by a growing population of elderly patients; those who lack proper housing; and those who lack family physicians to provide primary care. The Canadian Foundation for Healthcare Improvement projected a possible ED service utilization increase in Canada at a rate of 40% over three decades. This calls for local-level information on the time trends to understand demographic and temporal variations in the different geographical locations in the country. This study sought to identify and quantify acuity level-based per capita ED visit annual time trends for the 10-year period of 2006-2015 (by age, gender, and housing status). The aim is to provide detailed information on the time trends for demographically targeted ED planning locally. The lengthy record of data allows examining the changing directions in different time segments. Material and methods Administrative data from the largest emergency department in Halifax (Nova Scotia, Canada) was analyzed. Per capita adult ED visit rates (EDVR) based on Canadian Triage Acuity Scale (CTAS), age, gender, and housing status were analyzed. Trends in the age-gender-based standardized rates using 2011 census city population data were also estimated in order to account for the population increase in the city. Results No study in Canada has documented the possibility of flattening the escalating ED visit trend by maintaining an annual declining trend in low-acuity-level visits or documented a threshold rate of decline to be maintained. This study observed that the annual linear per capita non-homeless EDVR increment trend (328/year, CI:245-411, per 100,000) for all-acuity-level visits - noted for a ten-year period - would become stable when low-acuity-level CTAS4-5 visit declining trends (427/year, CI:350-503 and 121/year, CI:79-163, per 100,000) - noted for the period of 2012-2015 - were maintained at the same magnitude and direction Alarming annual emergent (high acuity level of CTAS2) EDVR increase equivalent to 335/year (CI:280-391, per 100,000) was noted for all combined visits, from all age, gender, and housing groups visits. The highest incremental rate noted among above-50-year-olds (521/year, per 100,000, 95% CI:433-608) was neither driven by overall increasing population census numbers nor by increasing aging population numbers. We found statistically similar age-gender standardized rates (294/year, CI: 207-382) for all ED visits and (316/year, CI:261-372) for CTAS2 level visits, when adjusted for annual population increase. Homeless ED visits did not contribute to the overall ED visit incremental trend. The highest annual homeless increment rate was shown for <30-year-old group high acuity CTAS-2 level visits (219/year, CI:193-246, per 100,000). Conclusion Neither the city population increase nor increased homeless visits contributed to ED visit annual per capita incremental trends in the city of Halifax. The increasing trend was chiefly driven by high-acuity-level visits by >50-year-old patients. Our findings suggest one way to make this escalating ED visit rates stable in the future is by maintaining the declining semi-urgent and non-urgent visit trends at the same rates estimated within the years 2012-2015. These findings highlight the potential directions for ED services planning to keep up with the growing demand for high-acuity-level ED services by the aging population.
引言 加拿大的急诊科正承受着越来越多老年患者、无适当住房者以及缺乏家庭医生提供初级护理者不断增加的就诊压力。加拿大医疗保健改善基金会预计,在未来三十年里,加拿大急诊科服务的利用率可能会以40%的速度增长。这就需要地方层面有关时间趋势的信息,以了解该国不同地理位置的人口和时间变化情况。本研究旨在确定并量化2006 - 2015年这十年间基于 acuity 水平的人均急诊科就诊年度时间趋势(按年龄、性别和住房状况)。目的是为地方层面针对特定人群的急诊科规划提供有关时间趋势的详细信息。长时间的数据记录使得能够研究不同时间段内的变化方向。
材料与方法 对加拿大新斯科舍省哈利法克斯最大的急诊科的行政数据进行了分析。分析了基于加拿大分诊 acuity 量表(CTAS)、年龄、性别和住房状况的成人急诊就诊率(EDVR)。还使用2011年人口普查城市人口数据估计了基于年龄 - 性别的标准化率趋势,以考虑城市人口的增长。
结果 加拿大尚无研究记录通过保持低 acuity 水平就诊的年度下降趋势来使不断上升的急诊就诊趋势趋于平缓的可能性,也没有记录需要维持的下降阈值率。本研究观察到,在2012 - 2015年期间记录到的低 acuity 水平CTAS4 - 5就诊下降趋势(每10万人每年分别为427次,CI:350 - 503;以及121次,CI:79 - 163)以相同的幅度和方向持续时,所有 acuity 水平就诊的年度线性人均非无家可归者EDVR增量趋势(每10万人每年328次,CI:245 - 411)在十年期间将趋于稳定。在所有年龄、性别和住房群体的综合就诊中,观察到年度急诊(CTAS2高 acuity 水平)EDVR的惊人增长,相当于每10万人每年增加335次(CI:280 - 391)。在50岁以上人群中观察到的最高增量率(每10万人每年521次,95%CI:433 - 608)既不是由总体人口普查数字的增加也不是由老年人口数量的增加所驱动。在考虑年度人口增长因素后,我们发现所有急诊就诊的年龄 - 性别标准化率在统计学上相似(每10万人每年294次,CI:207 - 382),CTAS2水平就诊的标准化率为(每10万人每年316次,CI:261 - 372)。无家可归者的急诊就诊对总体急诊就诊增量趋势没有贡献。在30岁以下年龄组的高 acuity CTAS - 2水平就诊中显示出最高的年度无家可归者增量率(每10万人每年219次,CI:193 - 246)。
结论 在哈利法克斯市,城市人口的增加和无家可归者就诊的增加都没有导致急诊就诊人均年度增量趋势。增长趋势主要由50岁以上患者的高 acuity 水平就诊所驱动。我们的研究结果表明,未来使这种不断上升的急诊就诊率趋于稳定的一种方法是保持2012 - 2015年期间估计的半紧急和非紧急就诊下降趋势。这些发现突出了急诊科服务规划的潜在方向,以满足老年人口对高 acuity 水平急诊科服务不断增长的需求。