Quansah Dan Yedu, Gross Justine, Mbundu-Ilunga Richard, Puder Jardena J
Obstetric Service, Department Woman-Mother-Child, Lausanne University Hospital, Lausanne Switzerland Avenue de la Sallaz, CH-1011, Lausanne, Switzerland.
Service of Endocrinology, Diabetes and Metabolism, Department of Medicine, Lausanne University Hospital, Lausanne, Switzerland.
Diabetol Metab Syndr. 2021 Mar 17;13(1):31. doi: 10.1186/s13098-021-00650-7.
Due to diverging international recommendations, the unclear role of HbA1c and the lack of longitudinal data, we investigated the accuracy of diagnostic tests in the early and late postpartum in women with gestational diabetes (GDM) especially to predict future glucose-intolerance.
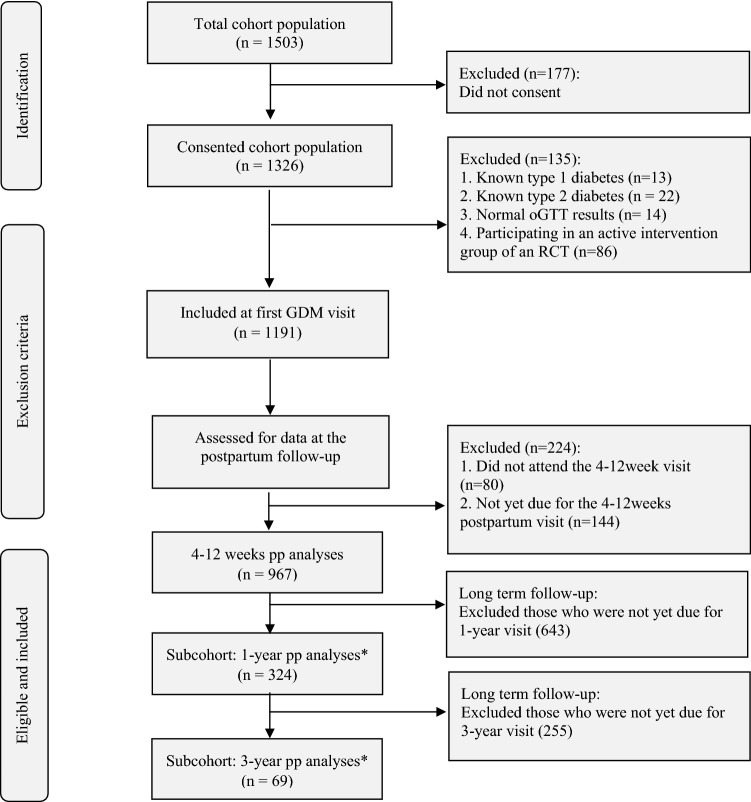
This longitudinal cohort included 967 women with GDM from 2011 to 2020. A 75-g oGTT and HbA1c were performed at 4-12 weeks (early) postpartum. FPG and HbA1c were measured at 1 and 3-year (late) postpartum. ADA criteria were used as gold standards. At all time-points (4-12 weeks, 1-year and 3-year postpartum) women with diabetes and prediabetes were grouped together and referred to as glucose-intolerant, because at most 3% of the entire cohort population had diabetes at any time-point.
The prevalence of glucose-intolerance in the early postpartum was higher using FPG and HbA1c (27.5%) than oGTT criteria (18.2%). Only 48-80% of women diagnosed with glucose-intolerance in the early postpartum actually remained intolerant. This was especially low when FPG or oGTT were combined with HbA1c (1-year: ≤ 62% and 3-years: ≤ 50%). Regardless of the test used, 1/3 of women with initially normal glucose-tolerance became glucose-intolerant in the late postpartum. HbA1c was unrelated to iron status/intake, remained stable throughout, but poorly predicted future glucose-intolerance. In the longitudinal analyses, all diagnostic tests in the early postpartum showed acceptable specificities (74-96%) but poor sensitivities (all < 38%) to predict glucose-intolerance after only 10-months. At 1-year postpartum however, the combination of FPG and HbA1c could best predict glucose-intolerance 2-years later.
Combining FPG with HbA1c at 1-year postpartum represents a reliable choice to predict future glucose-intolerance. Given the poor prediction of tests including oGTT in the early postpartum, focus should rather be on continuous long-term screening.
由于国际上的建议存在分歧、糖化血红蛋白(HbA1c)的作用不明确以及缺乏纵向数据,我们研究了妊娠期糖尿病(GDM)女性产后早期和晚期诊断测试的准确性,尤其是预测未来糖耐量异常的准确性。
该纵向队列研究纳入了2011年至2020年间的967例GDM女性。产后4 - 12周(早期)进行75克口服葡萄糖耐量试验(oGTT)和HbA1c检测。产后1年和3年(晚期)测量空腹血糖(FPG)和HbA1c。采用美国糖尿病协会(ADA)标准作为金标准。在所有时间点(产后4 - 12周、1年和3年),将患有糖尿病和糖尿病前期的女性归为一组,称为糖耐量异常,因为在整个队列人群中,任何时间点患糖尿病的比例最多为3%。
产后早期使用FPG和HbA1c诊断的糖耐量异常患病率(27.5%)高于oGTT标准(18.2%)。产后早期被诊断为糖耐量异常的女性中,实际仍处于糖耐量异常状态的仅占48% - 80%。当FPG或oGTT与HbA1c联合使用时,这一比例尤其低(产后1年:≤62%;产后3年:≤50%)。无论使用何种检测方法,最初糖耐量正常的女性中有1/3在产后晚期出现糖耐量异常。HbA1c与铁状态/铁摄入量无关,在整个过程中保持稳定,但对未来糖耐量异常的预测能力较差。在纵向分析中,产后早期所有诊断测试对预测仅10个月后的糖耐量异常显示出可接受的特异性(74% - 96%),但敏感性较差(均<38%)。然而,在产后1年时,FPG和HbA1c联合使用能最好地预测2年后的糖耐量异常。
产后1年时将FPG与HbA1c联合使用是预测未来糖耐量异常的可靠选择。鉴于产后早期包括oGTT在内的检测预测能力较差,应重点关注持续的长期筛查。