Provenzano Robert, Fishbane Steven, Szczech Lynda, Leong Robert, Saikali Khalil G, Zhong Ming, Lee Tyson T, Houser Mark T, Frison Lars, Houghton John, Little Dustin J, Peony Yu Kin-Hung, Neff Thomas B
School of Medicine, Wayne State University, Detroit, Michigan, USA.
Department of Medicine, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Great Neck, New York, USA.
Kidney Int Rep. 2020 Dec 24;6(3):613-623. doi: 10.1016/j.ekir.2020.12.018. eCollection 2021 Mar.
Erythropoiesis-stimulating agents are associated with increased cardiovascular risk when higher doses are used toward higher hematocrit targets. Patients new to dialysis are at higher risk for morbidity and mortality. Systematic evaluation of this population was predefined in the roxadustat clinical development program. Roxadustat is a hypoxia-inducible prolyl hydroxylase inhibitor.
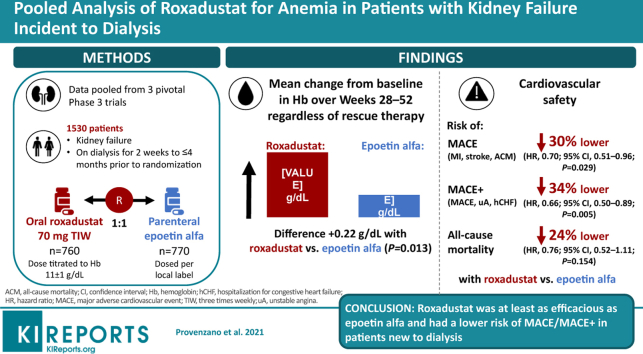
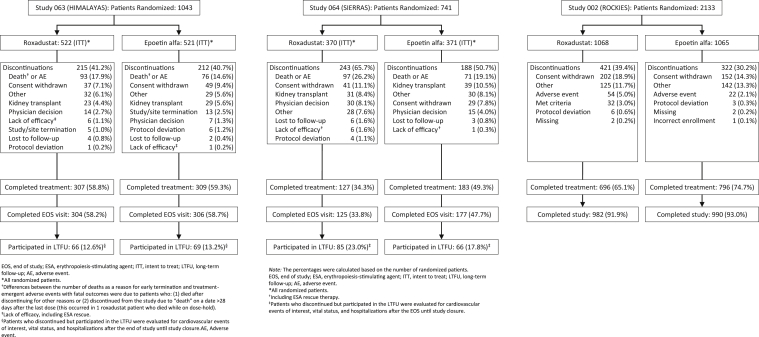
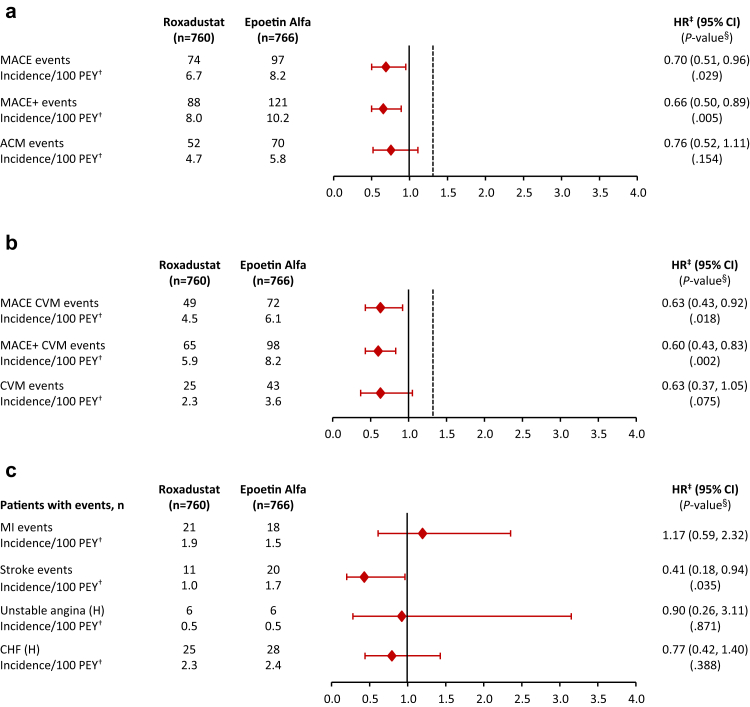
Data were pooled from 3 phase 3, randomized, open-label, active-controlled trials. Eligible adults had kidney failure and initiated dialysis for 2 weeks to ≤ 4 months prior to randomization to roxadustat or epoetin alfa. Efficacy was assessed as mean change in hemoglobin from baseline averaged over weeks 28 to 52, regardless of rescue therapy. Key cardiovascular safety endpoints were major adverse cardiovascular events (MACE; all-cause mortality [ACM], myocardial infarction, and stroke), and MACE+ (MACE plus unstable angina or congestive heart failure requiring hospitalization), and ACM.
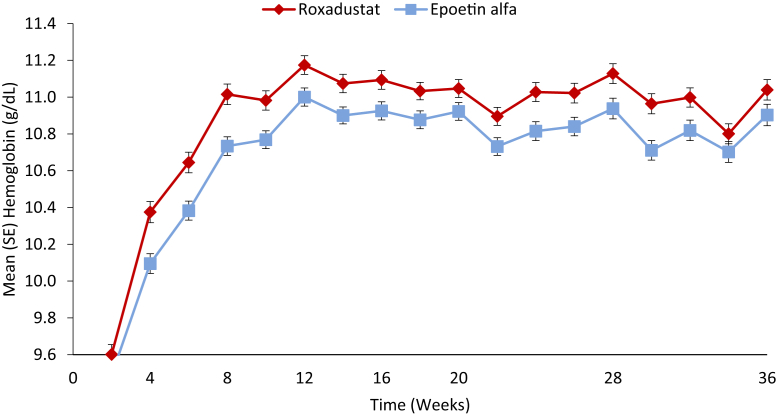
This study included 1530 patients with kidney failure incident to dialysis. Mean (SD) changes in hemoglobin from baseline averaged over weeks 28 to 52, regardless of rescue therapy, were 2.12 (1.45) versus 1.91 (1.42) g/dl in the roxadustat and epoetin alfa groups (least-squares mean difference: 0.22; 95% CI, 0.05 to 0.40; = 0.0130). Risks of MACE and MACE+ were lower in the roxadustat group (hazard ratio [HR], 0.70; 95% CI, 0.51 to 0.96) than the epoetin alfa group (HR, 0.66; 95% CI, 0.50 to 0.89); the HR for ACM was 0.76 (95% CI, 0.52 to 1.11).
Roxadustat was at least as efficacious as epoetin alfa. Roxadustat had a lower risk of MACE/MACE+ in patients new to dialysis.
当使用更高剂量以达到更高的血细胞比容目标时,促红细胞生成素与心血管风险增加相关。新开始透析的患者发生发病和死亡的风险更高。在罗沙司他临床开发项目中预先设定了对该人群的系统评估。罗沙司他是一种缺氧诱导脯氨酰羟化酶抑制剂。
数据来自3项3期随机、开放标签、活性对照试验。符合条件的成年人患有肾衰竭,在随机分组接受罗沙司他或促红细胞生成素α治疗前2周≤4个月开始透析。疗效评估为第28至52周血红蛋白相对于基线的平均变化,无论是否进行挽救治疗。关键心血管安全终点为主要不良心血管事件(MACE;全因死亡率[ACM]、心肌梗死和中风)、MACE+(MACE加不稳定型心绞痛或需要住院治疗的充血性心力衰竭)以及ACM。
本研究纳入了1530例新开始透析的肾衰竭患者。无论是否进行挽救治疗,罗沙司他组和促红细胞生成素α组第28至52周血红蛋白相对于基线的平均(标准差)变化分别为2.12(1.45)和1.91(1.42)g/dl(最小二乘平均差:0.22;95%置信区间,0.05至0.40;P = 0.0130)。罗沙司他组MACE和MACE+的风险低于促红细胞生成素α组(风险比[HR],0.70;95%置信区间,0.51至0.96);ACM的HR为0.76(95%置信区间,0.52至1.11)。
罗沙司他的疗效至少与促红细胞生成素α相当。罗沙司他在新开始透析的患者中发生MACE/MACE+的风险较低。