Department of Surgery Duke University Hospital Durham NC Department of MedicineDivision of Gastroenterology Duke University Hospital Durham NC Duke University School of Medicine Durham NC Division of NephrologyDepartment of Medicine Duke Unive Durham NC Division of HepatologyDepartment of Medicine Duke Unviersity Hospital Durham NC.
Liver Transpl. 2021 Aug;27(8):1106-1115. doi: 10.1002/lt.26053. Epub 2021 Jul 14.
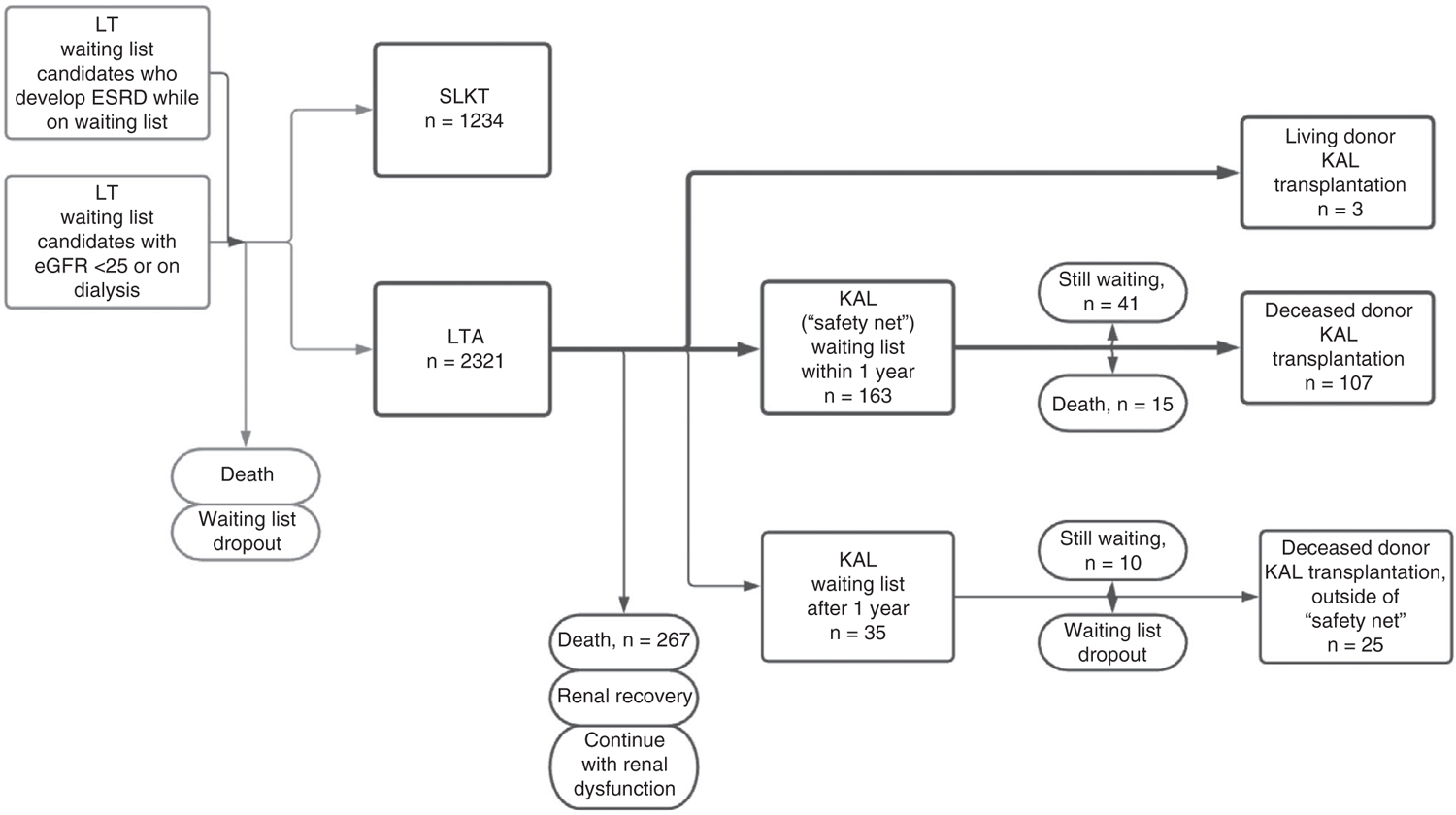
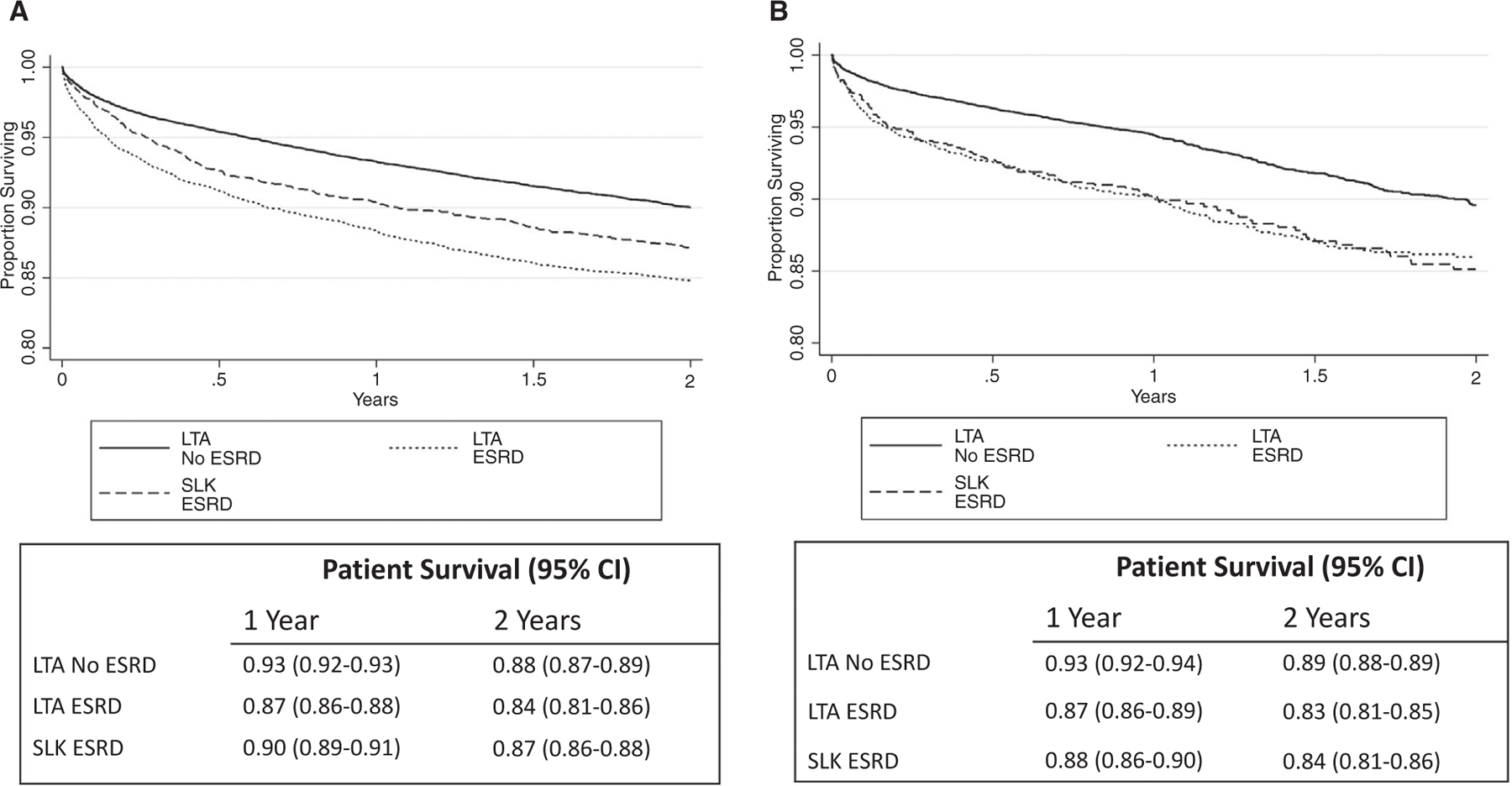
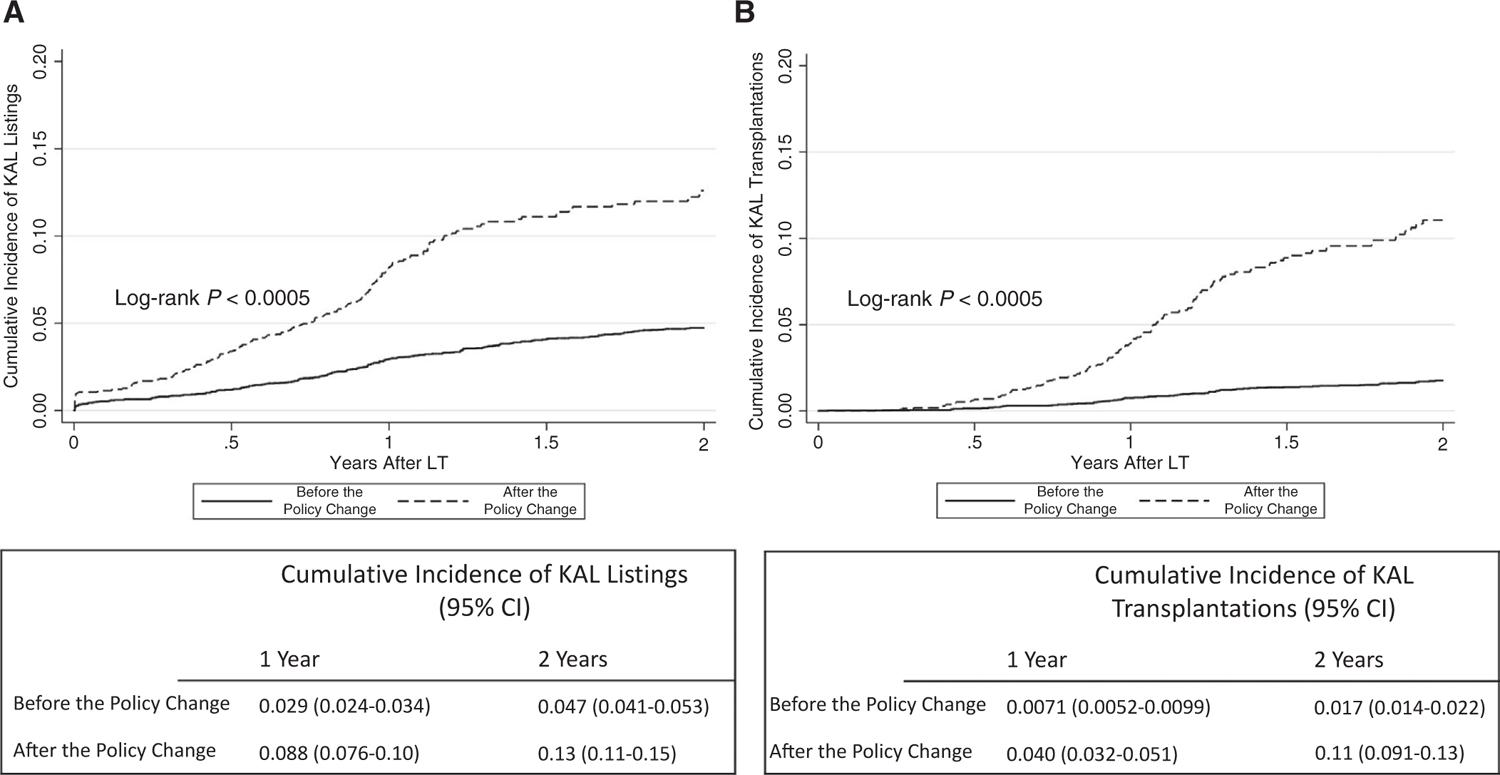
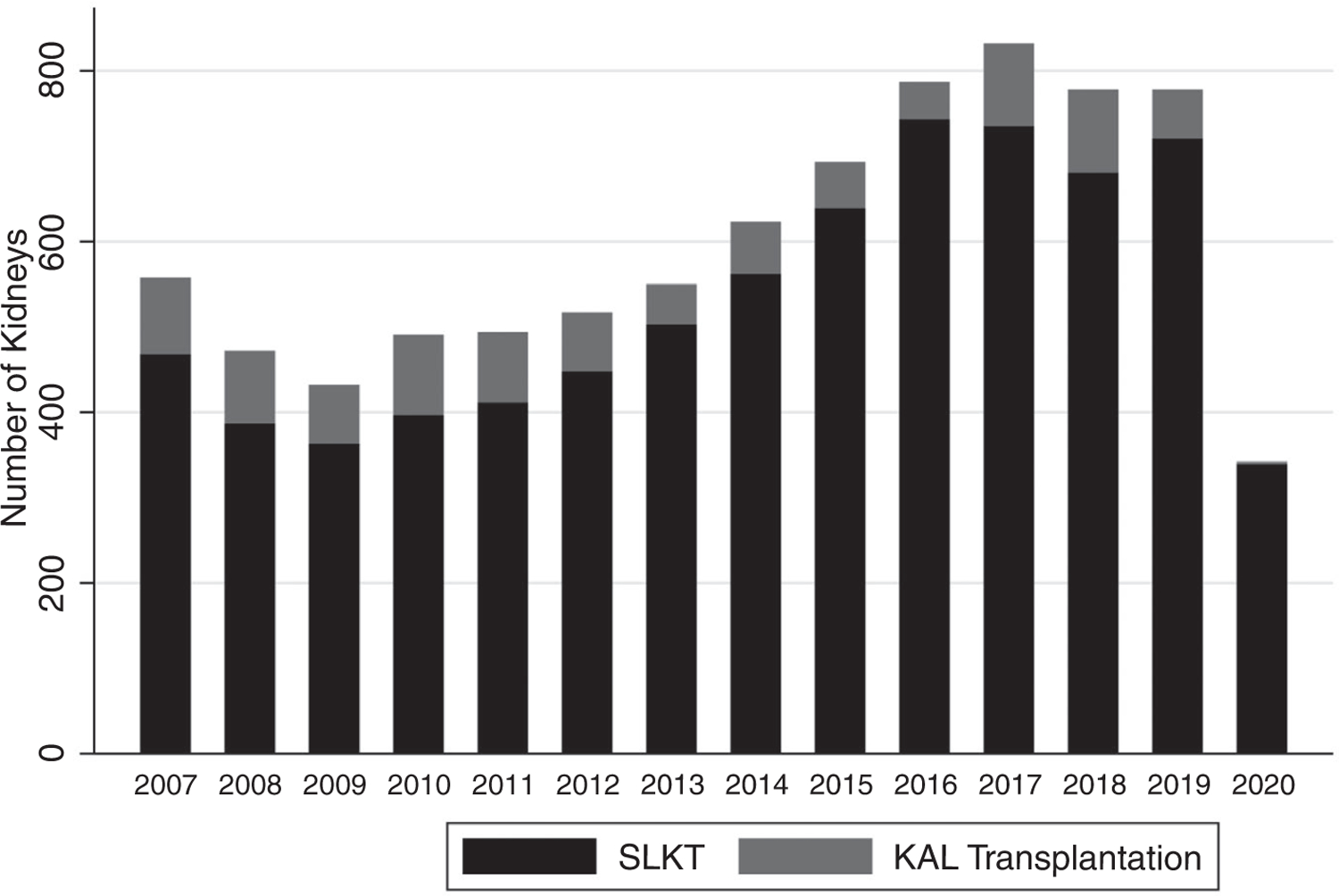
Historically in the United States, kidneys for simultaneous liver-kidney transplantation (SLKT) candidates were allocated with livers, prioritizing SLKT recipients over much of the kidney waiting list. A 2017 change in policy delineated renal function criteria for SLKT and implemented a safety net for kidney-after-liver transplantation. We compared the use and outcomes of SLKT and kidney-after-liver transplant with the 2017 policy. United Network for Organ Sharing Standard Transplant Analysis and Research files were used to identify adults who received liver transplantations (LT) from August 10, 2007 to August 10, 2012; from August 11, 2012 to August 10, 2017; and from August 11, 2017 to June 12, 2019. LT recipients with end-stage renal disease (ESRD) were defined by dialysis requirement or estimated glomerular filtration rate <25. We evaluated outcomes and center-level, regional, and national practice before and after the policy change. Nonparametric cumulative incidence of kidney-after-liver listing and transplant were modeled by era. A total of 6332 patients received SLKTs during the study period; fewer patients with glomerular filtration rate (GFR) ≥50 mL/min underwent SLKT over time (5.8%, 4.8%, 3.0%; P = 0.01 ). There was also less variability in GFR at transplant after policy implementation on center and regional levels. We then evaluated LT-alone (LTA) recipients with ESRD (n = 5408 from 2012-2017; n = 2321 after the policy). Listing for a kidney within a year of LT increased from 2.9% before the policy change to 8.8% after the policy change, and the rate of kidney transplantation within 1 year increased from 0.7% to 4% (P < 0.001). After the policy change, there was no difference in patient survival rates between SLKT and LTA among patients with ESRD. Implementation of the 2017 SLKT policy change resulted in reduced variability in SLKT recipient kidney function and increased access to deceased donor kidney transplantation for LTA recipients with kidney disease without negatively affecting outcomes.
在美国历史上,用于同时进行肝-肾移植 (SLKT) 的肾脏与肝脏一起分配,优先考虑 SLKT 受者,而将大部分肾脏候补名单上的人排在后面。2017 年的政策变化规定了 SLKT 的肾功能标准,并为肝移植后肾脏移植建立了安全网。我们比较了 2017 年政策前后 SLKT 和肝移植后肾脏的使用情况和结果。使用 United Network for Organ Sharing Standard Transplant Analysis and Research 文件,确定了 2007 年 8 月 10 日至 2012 年 8 月 10 日、2012 年 8 月 11 日至 2017 年 8 月 10 日以及 2017 年 8 月 11 日至 2019 年 6 月 12 日期间接受过肝脏移植 (LT) 的成年人。终末期肾病 (ESRD) 的 LT 受者通过透析要求或估计肾小球滤过率 <25 来定义。我们评估了政策变化前后的结果和中心水平、区域和国家实践。按时代对 SLKT 和肝移植后肾脏的列入和移植的非参数累积发生率进行建模。研究期间共有 6332 名患者接受了 SLKT;随着时间的推移,肾小球滤过率 (GFR)≥50 mL/min 的患者接受 SLKT 的人数减少 (5.8%、4.8%、3.0%;P=0.01)。在中心和区域层面上,政策实施后,移植时 GFR 的变异性也较小。然后,我们评估了 ESRD 的 LT 单独接受者 (LTA) (2012-2017 年有 5408 名患者;政策后有 2321 名患者)。LT 后一年内的肾脏清单数量从政策变化前的 2.9%增加到政策变化后的 8.8%,一年内的肾脏移植率从 0.7%增加到 4% (P<0.001)。政策变化后,ESRD 患者中 SLKT 和 LTA 的患者生存率没有差异。2017 年 SLKT 政策变化的实施减少了 SLKT 受者肾功能的变异性,并增加了对 LTA 受者的已故供体肾脏移植的机会,而没有对结果产生负面影响。