Department of Medicine D, Division of General Internal and Emergency Medicine, Nephrology, and Rheumatology, University Hospital Münster, Albert-Schweitzer-Campus 1, 48149, Münster, Germany.
Department of Cardiology and Angiology, University Hospital Münster, Albert-Schweitzer-Campus 1, 48149, Münster, Germany.
Crit Care. 2021 Mar 19;25(1):112. doi: 10.1186/s13054-021-03520-w.
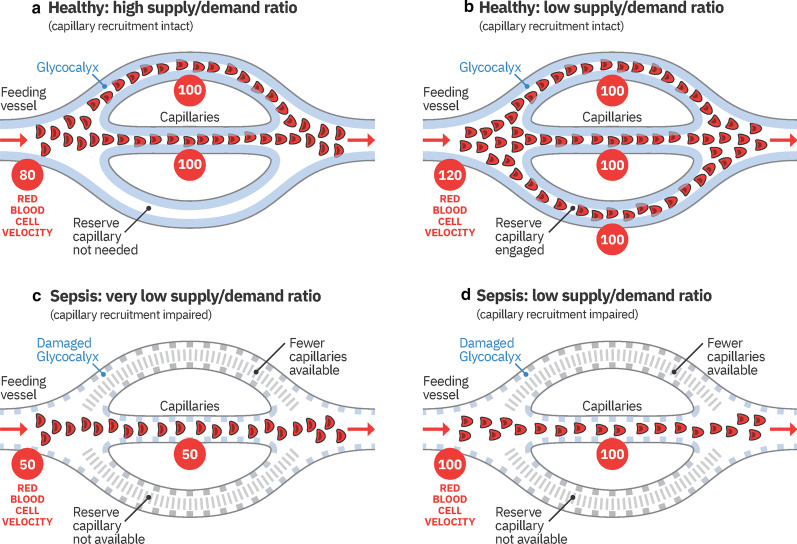
The availability of handheld, noninvasive sublingual video-microscopes allows for visualization of the microcirculation in critically ill patients. Recent studies demonstrate that reduced numbers of blood-perfused microvessels and increased penetration of erythrocytes into the endothelial glycocalyx are essential components of microvascular dysfunction. The aim of this study was to identify novel microvascular variables to determine the level of microvascular dysfunction in sepsis and its relationship with clinical variables.
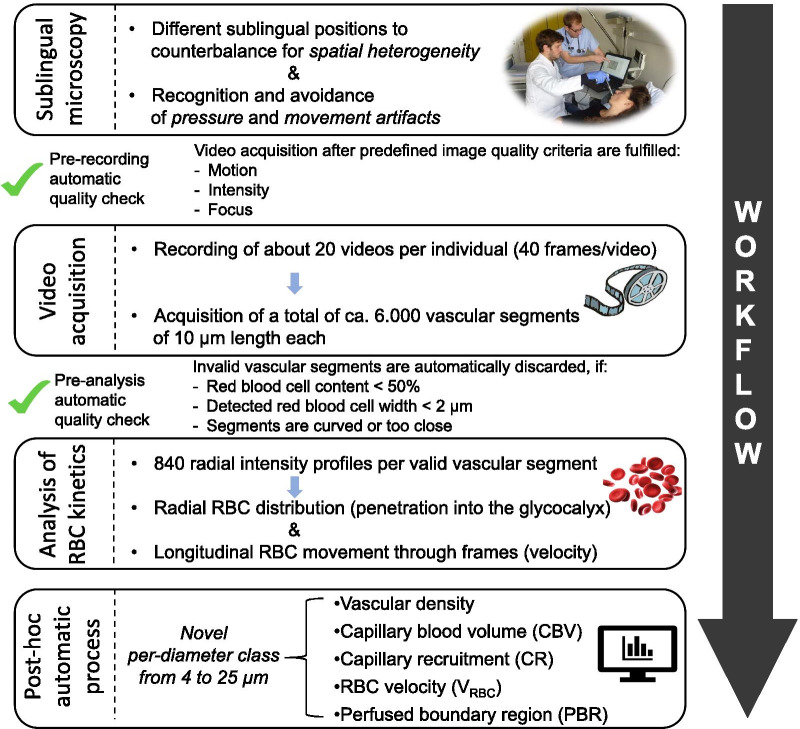
This observational, prospective, cross-sectional study included 51 participants, of which 34 critically ill sepsis patients were recruited from intensive care units of a university hospital. Seventeen healthy volunteers served as controls. All participants underwent sublingual videomicroscopy by sidestream darkfield imaging. A new developed version of the Glycocheck™ software was used to quantify vascular density, perfused boundary region (PBR-an inverse variable of endothelial glycocalyx dimensions), red blood cell (RBC) velocity, RBC content, and blood flow in sublingual microvessels with diameters between 4 and 25 µm.
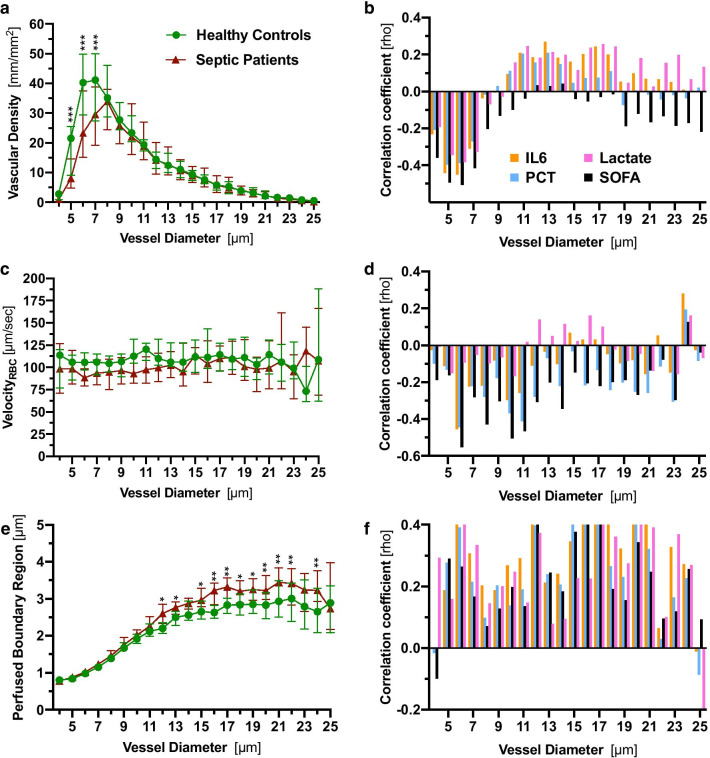
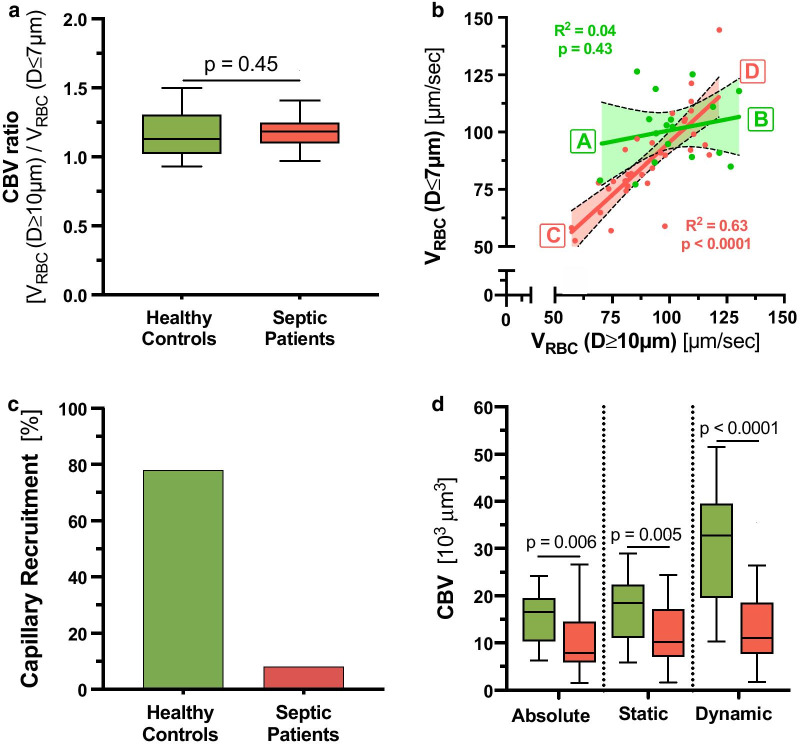
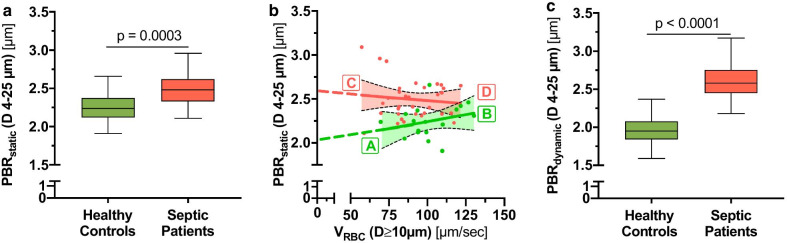
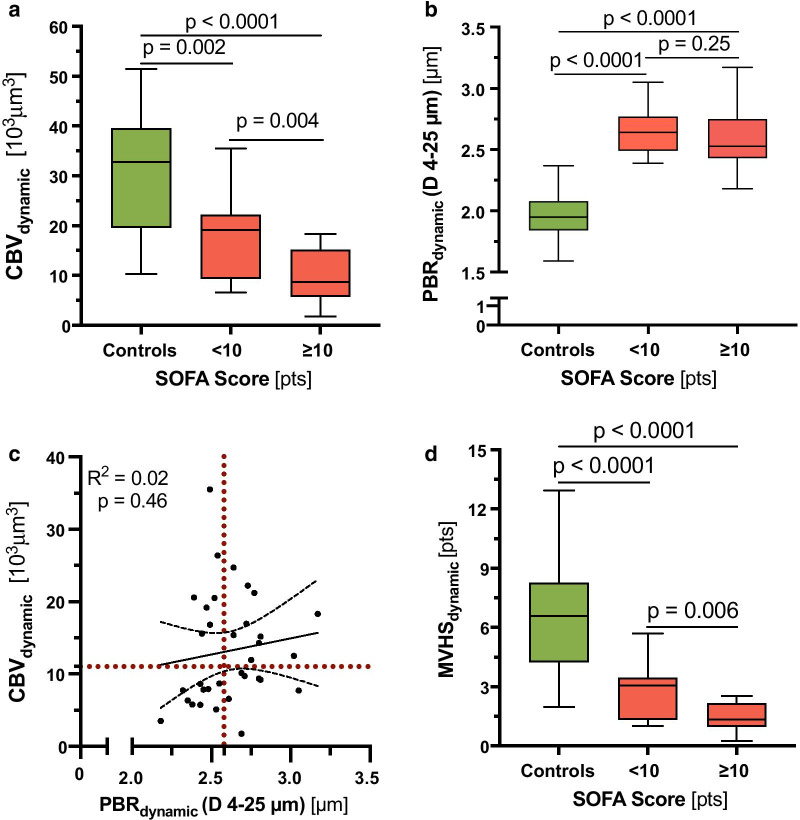
A detailed analysis of adjacent diameter classes (1 µm each) of vessels between 4 and 25 µm revealed a severe reduction of vascular density in very small capillaries (5-7 µm), which correlated with markers of sepsis severity. Analysis of RBC velocity (V) revealed a strong dependency between capillary and feed vessel V in sepsis patients (R = 0.63, p < 0.0001) but not in healthy controls (R = 0.04, p = 0.43), indicating impaired capillary (de-)recruitment in sepsis. This finding enabled the calculation of capillary recruitment and dynamic capillary blood volume (CBV). Moreover, adjustment of PBR to feed vessel V further improved discrimination between sepsis patients and controls by about 50%. By combining these dynamic microvascular and glycocalyx variables, we developed the microvascular health score (MVHS™), which decreased from 7.4 [4.6-8.7] in controls to 1.8 [1.4-2.7] in sepsis patients (p < 0.0001) and correlated with sepsis severity.
We introduce new important diameter-specific quantification and differentiated analysis of RBC kinetics, a key to understand microvascular dysfunction in sepsis. MVHS, which has a broad bandwidth to detect microvascular (dys-) function, might serve as a valuable tool to detect microvascular impairment in critically ill patients.
手持式、非侵入性舌下视频显微镜的出现使得对危重病患者的微循环进行可视化成为可能。最近的研究表明,血流灌注的微血管数量减少和红细胞穿透内皮糖萼增加是微血管功能障碍的重要组成部分。本研究旨在确定新的微血管变量,以确定脓毒症的微血管功能障碍程度及其与临床变量的关系。
本观察性、前瞻性、横断面研究纳入了 51 名参与者,其中 34 名危重病脓毒症患者从一所大学医院的重症监护病房招募。17 名健康志愿者作为对照组。所有参与者均接受舌下视频显微镜检查,采用边流暗场成像。使用新开发的 Glycocheck™软件版本来量化血管密度、灌注边界区域(PBR-内皮糖萼尺寸的逆变量)、红细胞(RBC)速度、RBC 含量和直径在 4 至 25 µm 之间的舌下微血管中的血流。
对直径为 4 至 25 µm 的相邻直径类别的详细分析(每个 1 µm)表明,非常小的毛细血管(5-7 µm)的血管密度严重降低,这与脓毒症严重程度的标志物相关。RBC 速度(V)的分析表明,在脓毒症患者中,毛细血管和供血血管 V 之间存在强烈的依赖性(R=0.63,p<0.0001),而在健康对照组中则没有(R=0.04,p=0.43),这表明脓毒症患者的毛细血管(去)募集受损。这一发现使计算毛细血管募集和动态毛细血管血容量(CBV)成为可能。此外,将 PBR 调整到供血血管 V 进一步将脓毒症患者和对照组之间的区分度提高了约 50%。通过结合这些动态微血管和糖萼变量,我们开发了微血管健康评分(MVHS™),该评分从对照组的 7.4 [4.6-8.7]降至脓毒症患者的 1.8 [1.4-2.7](p<0.0001),并与脓毒症严重程度相关。
我们引入了新的重要的直径特异性 RBC 动力学定量和差异化分析,这是理解脓毒症中微血管功能障碍的关键。MVHS 具有广泛的带宽来检测微血管(功能)障碍,可能是检测危重病患者微血管损伤的有用工具。