Department of Cardiology, Rigshospitalet, Copenhagen University Hospital, Denmark (M.A.S.M., S.W., J.G., A.S.P.M., M.F., J.H.T., J.J., J.E.M., J.K., C.H.).
Department of Cardiology, Odense University Hospital, Denmark (J.E.M.).
Circulation. 2021 May 11;143(19):1841-1851. doi: 10.1161/CIRCULATIONAHA.120.053318. Epub 2021 Mar 22.
Patients experiencing out-of-hospital cardiac arrest who remain comatose after initial resuscitation are at high risk of morbidity and mortality attributable to the ensuing post-cardiac arrest syndrome. Systemic inflammation constitutes a major component of post-cardiac arrest syndrome, and IL-6 (interleukin-6) levels are associated with post-cardiac arrest syndrome severity. The IL-6 receptor antagonist tocilizumab could potentially dampen inflammation in post-cardiac arrest syndrome. The objective of the present trial was to determine the efficacy of tocilizumab to reduce systemic inflammation after out-of-hospital cardiac arrest of a presumed cardiac cause and thereby potentially mitigate organ injury.
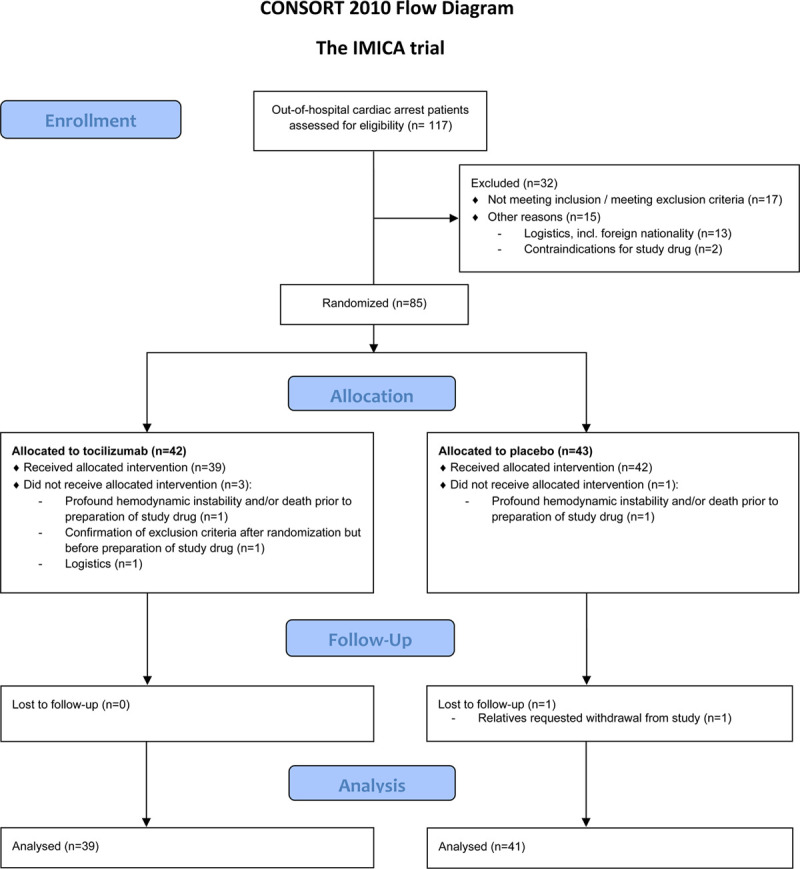
Eighty comatose patients with out-of-hospital cardiac arrest were randomly assigned 1:1 in a double-blinded placebo-controlled trial to a single infusion of tocilizumab or placebo in addition to standard of care including targeted temperature management. Blood samples were sequentially drawn during the initial 72 hours. The primary end point was the reduction in C-reactive protein response from baseline until 72 hours in patients treated with tocilizumab evaluated by mixed-model analysis for a treatment-by-time interaction. Secondary end points (main) were the marker of inflammation: leukocytes; the markers of myocardial injury: creatine kinase myocardial band, troponin T, and N-terminal pro B-type natriuretic peptide; and the marker of brain injury: neuron-specific enolase. These secondary end points were analyzed by mixed-model analysis.
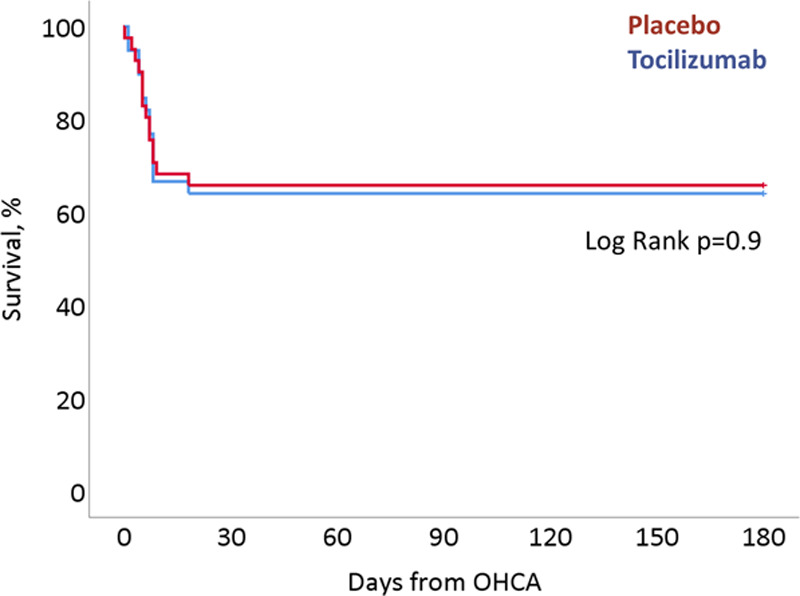
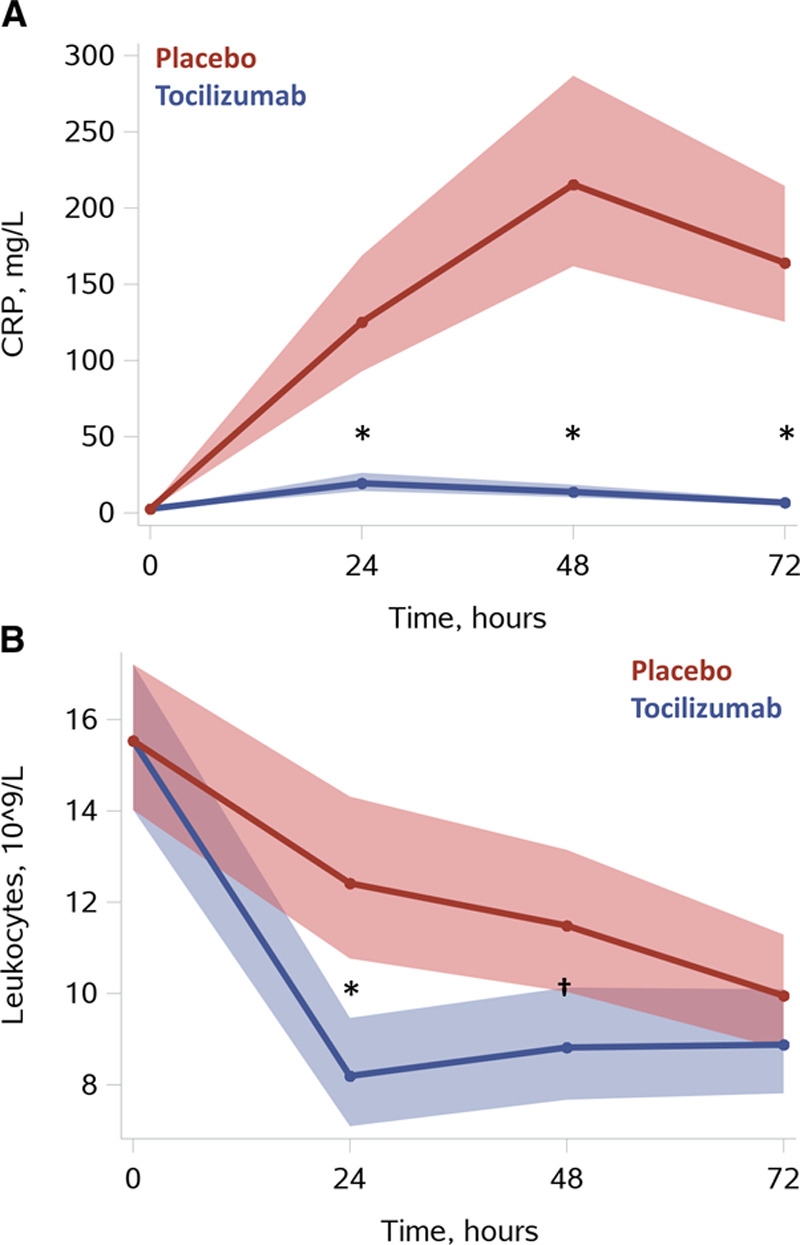
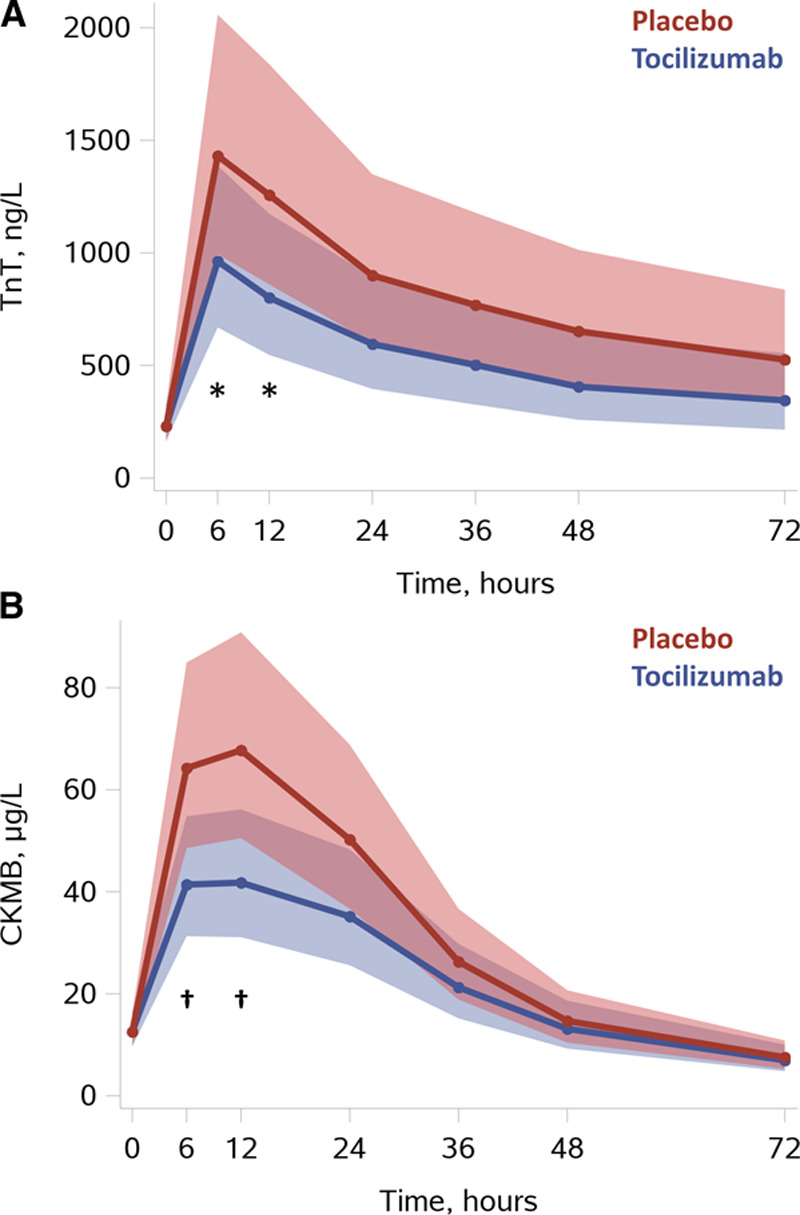
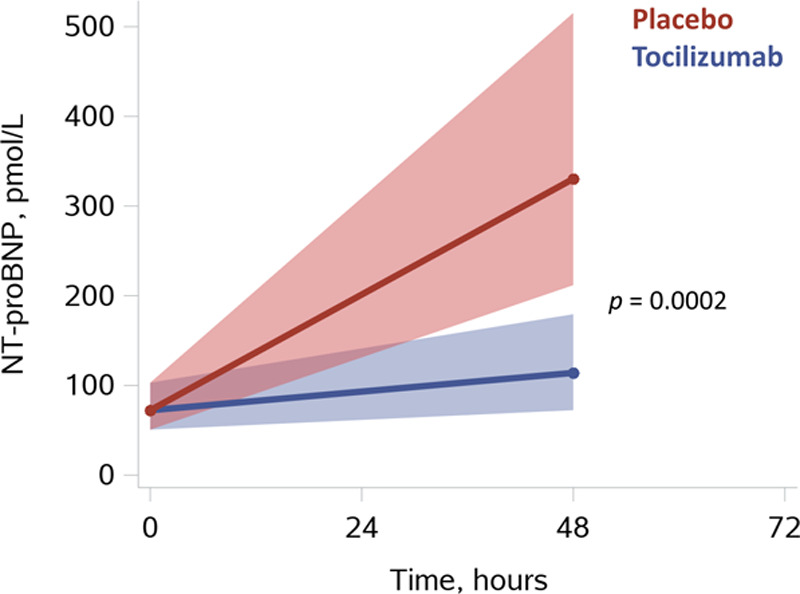
The primary end point of reducing the C-reactive protein response by tocilizumab was achieved since there was a significant treatment-by-time interaction, <0.0001, and a profound effect on C-reactive protein levels. Systemic inflammation was reduced by treatment with tocilizumab because both C-reactive protein and leukocyte levels were markedly reduced, tocilizumab versus placebo at 24 hours: -84% [-90%; -76%] and -34% [-46%; -19%], respectively, both <0.001. Myocardial injury was also reduced, documented by reductions in creatine kinase myocardial band and troponin T; tocilizumab versus placebo at 12 hours: -36% [-54%; -11%] and -38% [-53%; -19%], respectively, both <0.01. N-terminal pro B-type natriuretic peptide was similarly reduced by active treatment; tocilizumab versus placebo at 48 hours: -65% [-80%; -41%], <0.001. There were no differences in survival or neurological outcome.
Treatment with tocilizumab resulted in a significant reduction in systemic inflammation and myocardial injury in comatose patients resuscitated from out-of-hospital cardiac arrest. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03863015.
初始复苏后仍处于昏迷状态的院外心脏骤停患者存在高发病率和死亡率的风险,这与随后的心脏骤停后综合征有关。全身炎症是心脏骤停后综合征的一个主要组成部分,白细胞介素 6(IL-6)水平与心脏骤停后综合征的严重程度相关。IL-6 受体拮抗剂托珠单抗可能会减弱心脏骤停后的炎症反应。本试验的目的是确定托珠单抗是否能降低院外心脏骤停(推定心源性)后全身炎症反应,从而减轻器官损伤。
80 例昏迷的院外心脏骤停患者以 1:1 的比例随机分配到双盲安慰剂对照试验中,在标准治疗(包括目标温度管理)的基础上,接受单次托珠单抗或安慰剂输注。在最初的 72 小时内,连续采集血液样本。通过混合模型分析评估治疗时间的相互作用,以确定主要终点:在托珠单抗治疗组中,C 反应蛋白从基线到 72 小时的反应降低。次要终点(主要)为炎症标志物:白细胞;心肌损伤标志物:肌酸激酶心肌带、肌钙蛋白 T 和 N 端脑利钠肽前体;以及脑损伤标志物:神经元特异性烯醇化酶。这些次要终点通过混合模型分析进行评估。
托珠单抗达到了降低 C 反应蛋白反应的主要终点,因为存在显著的治疗时间相互作用,<0.0001,并且对 C 反应蛋白水平有显著影响。托珠单抗治疗降低了全身炎症反应,因为 C 反应蛋白和白细胞水平都明显降低,24 小时时托珠单抗与安慰剂相比:-84%[-90%;-76%]和-34%[-46%;-19%],均<0.001。肌酸激酶心肌带和肌钙蛋白 T 也显示心肌损伤减少,托珠单抗与安慰剂相比,在 12 小时时:-36%[-54%;-11%]和-38%[-53%;-19%],均<0.01。N 端脑利钠肽前体也通过积极治疗得到了类似的降低;托珠单抗与安慰剂相比,在 48 小时时:-65%[-80%;-41%],<0.001。两组之间在生存率或神经结局方面没有差异。
托珠单抗治疗可显著降低院外心脏骤停复苏后昏迷患者的全身炎症反应和心肌损伤。