Department of Gastroenterology and Hepatology, Sapporo Medical University, Japan.
Department of Medical Genetics, Sapporo Medical University, Japan.
Intern Med. 2021 Sep 1;60(17):2719-2724. doi: 10.2169/internalmedicine.6603-20. Epub 2021 Mar 22.
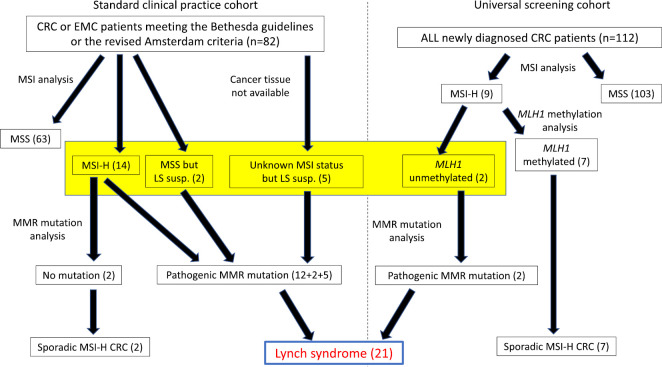
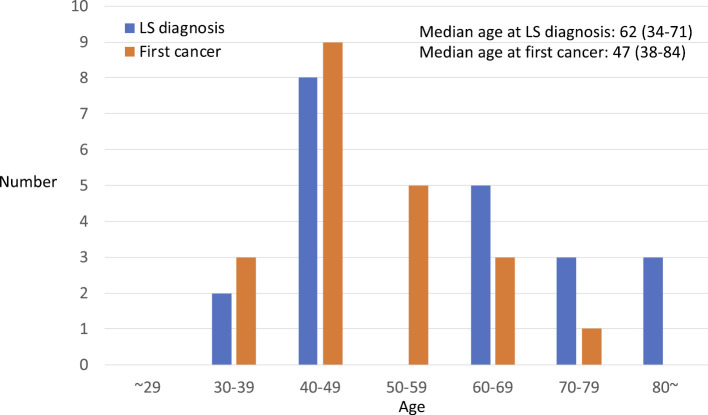
Objective Little is known about the time from developing a first cancer to confirming the presence of a mismatch repair (MMR) gene mutation for Lynch syndrome (LS) probands. Methods This was a retrospective single center study. LS probands, who have an MMR gene mutation that was confirmed first in a pedigree and thereafter developed at least one cancer, were included in this study. Results There were 21 LS probands who had developed at least one cancer; 6 with MLH1 mutations, 9 with MSH2 mutations, 4 with MSH6 mutations, and 2 with EPCAM deletions. The median ages at the first cancer and the genetic diagnosis were 47 (34-71) and 62 (38-84) years old, respectively. The mean interval between the first cancer and the genetic diagnosis was 11.0 (0-25) years, and 20 years or longer interval was required for the 5 probands. Six (28.6%) probands were older than 70 years, and 3 (14.3%) were in their 80s when they were diagnosed to have LS. The genetic diagnosis was confirmed at the first, second, third, and fourth cancer or later in 5, 5, 6, and 5 probands, respectively. Of the 16 cancers examined, 2 (12.5%) were microsatellite stable (MSS), both of whom had germline MSH6 mutations. All 17 LS probands who developed colorectal cancer met the revised Bethesda guidelines at the genetic diagnosis, but only 7 of 11 (63.6%) met them at the first cancer. Twelve out of 21 (57.1%) met the revised Amsterdam criteria. Conclusion It took 11 years for the LS probands from the first cancer to the diagnostic confirmation by genetic tests. A quarter of the probands were in their 70s or 80s at genetic diagnosis.
对于林奇综合征(LS)先证者,从首次罹患癌症到证实错配修复(MMR)基因突变的时间尚不清楚。
这是一项回顾性单中心研究。本研究纳入了在一个家系中首先证实存在 MMR 基因突变,随后至少罹患一种癌症的 LS 先证者。
共有 21 例 LS 先证者至少罹患了一种癌症;其中 6 例存在 MLH1 基因突变,9 例存在 MSH2 基因突变,4 例存在 MSH6 基因突变,2 例存在 EPCAM 缺失。首次癌症和遗传诊断的中位年龄分别为 47(34-71)岁和 62(38-84)岁。首次癌症与遗传诊断的平均间隔为 11.0(0-25)年,5 例先证者的间隔达到 20 年或更长。6 例(28.6%)先证者年龄超过 70 岁,3 例(14.3%)在 80 多岁时被诊断为 LS。5 例先证者的遗传诊断分别在首次、第二次、第三次和第四次癌症或更晚时得到证实,6 例先证者的遗传诊断在确诊为 LS 前已发生 2 次或更多次癌症。在 16 例癌症中,2 例(12.5%)为微卫星稳定(MSS),两者均存在胚系 MSH6 基因突变。所有 17 例发生结直肠癌的 LS 先证者在遗传诊断时均符合修订后的贝塞斯达指南,但仅 11 例(63.6%)在首次癌症时符合该指南。12/21(57.1%)例符合修订后的阿姆斯特丹标准。
LS 先证者从首次癌症到基因检测确诊需要 11 年。四分之一的先证者在遗传诊断时已 70 多岁或 80 多岁。