Department of Radiology and Nuclear Medicine, Maastricht UMC+, Maastricht, The Netherlands.
Department of Cardiology, Maastricht UMC+, Maastricht, The Netherlands.
J Cardiovasc Magn Reson. 2021 Mar 22;23(1):40. doi: 10.1186/s12968-021-00723-6.
Invasive coronary angiography (ICA) is still the reference test in suspected non-ST elevation myocardial infarction (NSTEMI), although a substantial number of patients do not have obstructive coronary artery disease (CAD). Early cardiovascular magnetic resonance (CMR) may be a useful gatekeeper for ICA in this setting. The main objective was to investigate the accuracy of CMR to detect obstructive CAD in NSTEMI.
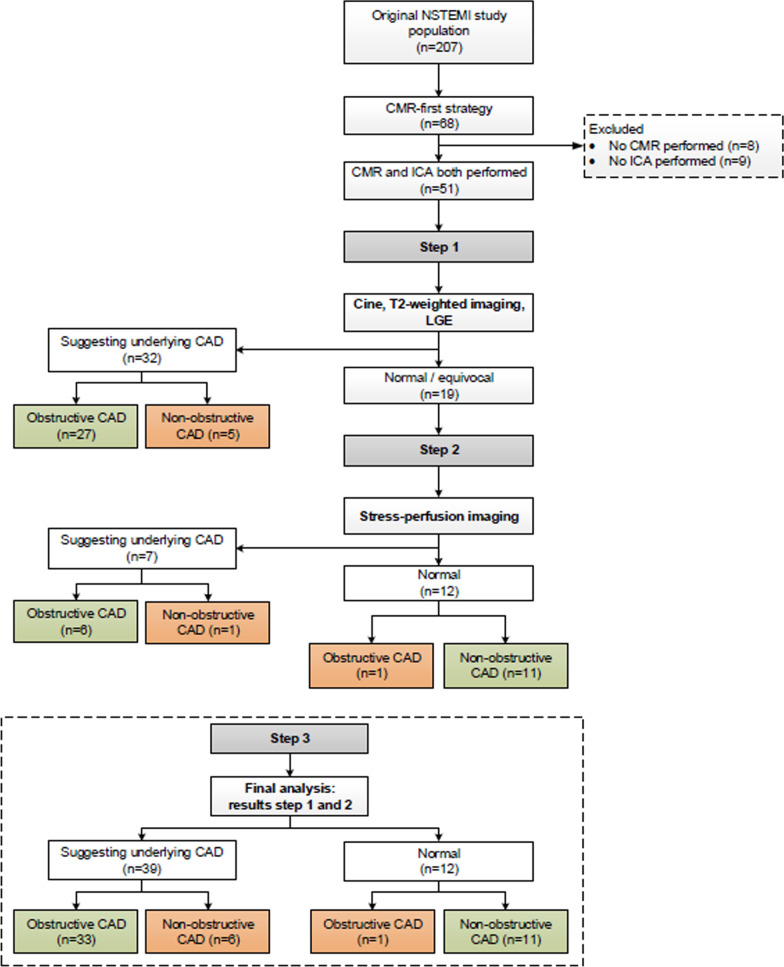
This study is a sub-analysis of a randomized controlled trial investigating whether a non-invasive imaging-first strategy safely reduced the number of ICA compared to routine clinical care in suspected NSTEMI (acute chest pain, non-diagnostic electrocardiogram, high sensitivity troponin T > 14 ng/L), and included 51 patients who underwent CMR prior to ICA. A stepwise approach was used to assess the diagnostic accuracy of CMR to detect (1) obstructive CAD (diameter stenosis ≥ 70% by ICA) and (2) an adjudicated final diagnosis of acute coronary syndrome (ACS). First, in all patients the combination of cine, T2-weighted and late gadolinium enhancement (LGE) imaging was evaluated for the presence of abnormalities consistent with a coronary etiology in any sequence. Hereafter and only when the scan was normal or equivocal, adenosine stress-perfusion CMR was added.
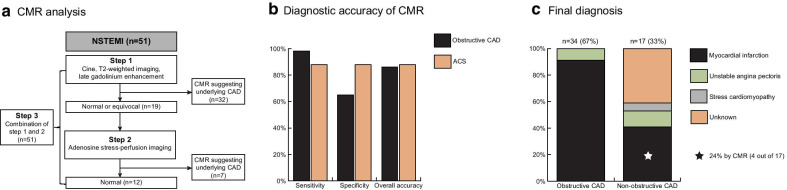
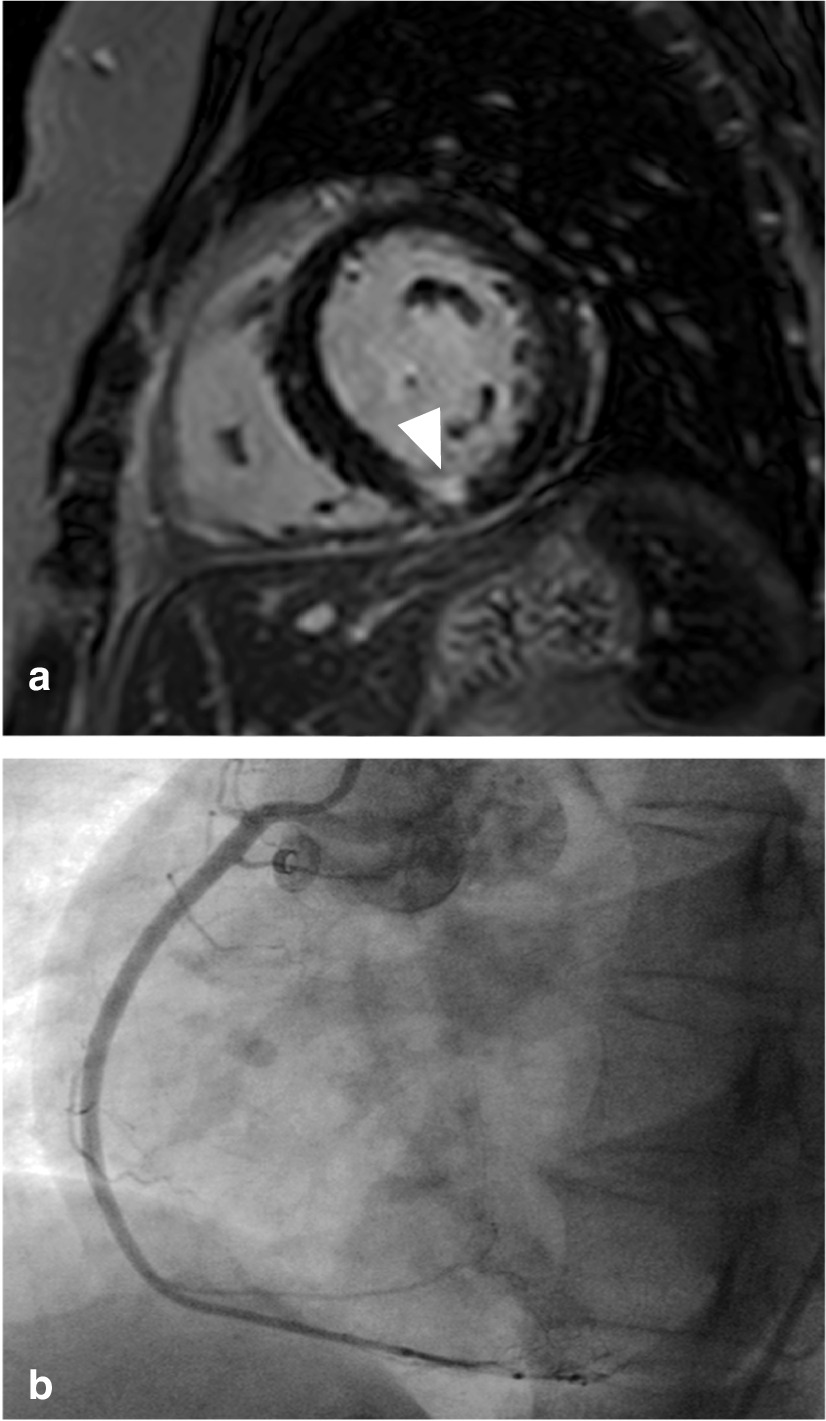
Of 51 patients included (63 ± 10 years, 51% male), 34 (67%) had obstructive CAD by ICA. The sensitivity, specificity and overall accuracy of the first step to diagnose obstructive CAD were 79%, 71% and 77%, respectively. Additional vasodilator stress-perfusion CMR was performed in 19 patients and combined with step one resulted in an overall sensitivity of 97%, specificity of 65% and accuracy of 86%. Of the remaining 17 patients with non-obstructive CAD, 4 (24%) had evidence for a myocardial infarction on LGE, explaining the modest specificity. The sensitivity, specificity and overall accuracy to diagnose ACS (n = 43) were 88%, 88% and 88%, respectively.
CMR accurately detects obstructive CAD and ACS in suspected NSTEMI. Non-obstructive CAD is common with CMR still identifying an infarction in almost one-quarter of patients. CMR should be considered as an early diagnostic approach in suspected NSTEMI.
The CARMENTA trial has been registered at ClinicalTrials.gov with identifier NCT01559467.
尽管大量患者不存在阻塞性冠状动脉疾病(CAD),但在疑似非 ST 段抬高型心肌梗死(NSTEMI)中,有创冠状动脉造影(ICA)仍然是参考检测手段。早期心血管磁共振(CMR)可能是该情况下 ICA 的一种有用的门控检测手段。主要目的是研究 CMR 检测 NSTEMI 中阻塞性 CAD 的准确性。
本研究为一项随机对照试验的子分析,该试验旨在探讨在疑似 NSTEMI(急性胸痛、非诊断性心电图、高敏肌钙蛋白 T > 14ng/L)中,与常规临床护理相比,非侵入性影像学优先策略是否能安全减少 ICA 的数量,共纳入 51 例在 ICA 前接受 CMR 检查的患者。采用逐步方法评估 CMR 检测(1)阻塞性 CAD(ICA 直径狭窄≥70%)和(2)经裁决的急性冠状动脉综合征(ACS)最终诊断的诊断准确性。首先,在所有患者中,评估电影、T2 加权和晚期钆增强(LGE)成像组合是否存在与冠状动脉病因一致的异常。此后,仅当扫描正常或不确定时,才会添加腺苷应激灌注 CMR。
共纳入 51 例患者(63±10 岁,51%为男性),其中 34 例(67%)ICA 显示阻塞性 CAD。第一阶段诊断阻塞性 CAD 的敏感性、特异性和总体准确性分别为 79%、71%和 77%。19 例患者进行了额外的血管扩张剂应激灌注 CMR,与第一步结合使用,总体敏感性为 97%,特异性为 65%,准确性为 86%。在其余 17 例非阻塞性 CAD 患者中,4 例(24%)LGE 显示有心肌梗死,这解释了特异性略低的原因。诊断 ACS(n=43)的敏感性、特异性和总体准确性分别为 88%、88%和 88%。
CMR 可准确检测疑似 NSTEMI 中的阻塞性 CAD 和 ACS。CMR 中常见非阻塞性 CAD,近四分之一的患者仍可检测到梗死。CMR 应考虑作为疑似 NSTEMI 的早期诊断方法。
CARMENTA 试验已在 ClinicalTrials.gov 注册,标识符为 NCT01559467。