University of Oxford Centre for Clinical Magnetic Resonance Research, Division of Cardiovascular Medicine, Radcliffe Department of Medicine, University of Oxford, Oxford, UK.
Department of Cardiovascular Sciences, University of Leicester, Leicester, UK.
J Cardiovasc Magn Reson. 2017 Oct 25;19(1):81. doi: 10.1186/s12968-017-0397-8.
Type 2 diabetes mellitus (T2DM) is associated with coronary microvascular dysfunction in the absence of obstructive coronary artery disease (CAD). Cardiovascular magnetic resonance (CMR) T1-mapping at rest and during adenosine stress can assess coronary vascular reactivity. We hypothesised that the non-contrast T1 response to vasodilator stress will be altered in patients with T2DM without CAD compared to controls due to coronary microvascular dysfunction.
Thirty-one patients with T2DM and sixteen matched healthy controls underwent CMR (3 T) for cine, rest and adenosine stress non-contrast T1-mapping (ShMOLLI), first-pass perfusion and late gadolinium enhancement (LGE) imaging. Significant CAD (>50% coronary luminal stenosis) was excluded in all patients by coronary computed tomographic angiography.
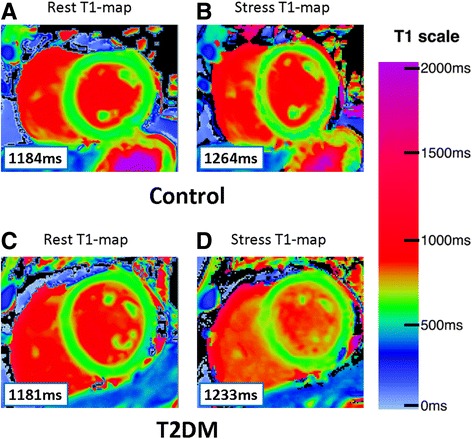
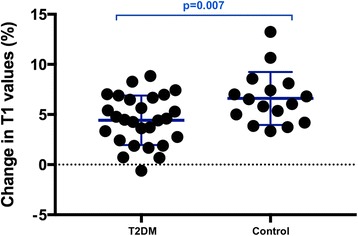
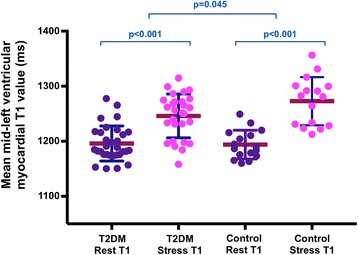
All subjects had normal left ventricular (LV) ejection and LV mass index, with no LGE. Myocardial perfusion reserve index (MPRI) was lower in T2DM than in controls (1.60 ± 0.44 vs 2.01 ± 0.42; p = 0.008). There was no difference in rest native T1 values (p = 0.59). During adenosine stress, T1 values increased significantly in both T2DM patients (from 1196 ± 32 ms to 1244 ± 44 ms, p < 0.001) and controls (from 1194 ± 26 ms to 1273 ± 44 ms, p < 0.001). T2DM patients showed blunted relative stress non-contrast T1 response (T2DM: ΔT1 = 4.1 ± 2.9% vs.
ΔT1 = 6.6 ± 2.6%, p = 0.007) due to a blunted maximal T1 during adenosine stress (T2DM 1244 ± 44 ms vs. controls 1273 ± 44 ms, p = 0.045).
Patients with well controlled T2DM, even in the absence of arterial hypertension and significant CAD, exhibit blunted maximal non-contrast T1 response during adenosine vasodilatory stress, likely reflecting coronary microvascular dysfunction. Adenosine stress and rest T1 mapping can detect subclinical abnormalities of the coronary microvasculature, without the need for gadolinium contrast agents. CMR may identify early features of the diabetic heart phenotype and subclinical cardiac risk markers in patients with T2DM, providing an opportunity for early therapeutic intervention.
2 型糖尿病(T2DM)与无阻塞性冠状动脉疾病(CAD)的冠状动脉微血管功能障碍有关。静息和腺苷应激时的心血管磁共振(CMR)T1 映射可评估冠状动脉血管反应性。我们假设,与对照组相比,由于冠状动脉微血管功能障碍,无 CAD 的 T2DM 患者在接受血管扩张剂应激时的非对比 T1 反应会发生改变。
31 例 T2DM 患者和 16 例匹配的健康对照组接受 CMR(3T)电影、静息和腺苷应激非对比 T1 映射(ShMOLLI)、首过灌注和晚期钆增强(LGE)成像。所有患者均通过冠状动脉计算机断层血管造影排除了 >50%的冠状动脉腔狭窄的显著 CAD。
所有受试者的左心室(LV)射血分数和 LV 质量指数均正常,无 LGE。与对照组相比,T2DM 患者的心肌灌注储备指数(MPRI)较低(1.60±0.44 vs 2.01±0.42;p=0.008)。静息时的原生 T1 值无差异(p=0.59)。在腺苷应激下,T2DM 患者的 T1 值(从 1196±32ms 增加到 1244±44ms,p<0.001)和对照组(从 1194±26ms 增加到 1273±44ms,p<0.001)均显著增加。T2DM 患者的相对应激非对比 T1 反应减弱(T2DM:ΔT1=4.1±2.9% vs.
ΔT1=6.6±2.6%,p=0.007),这是由于腺苷应激时最大 T1 降低(T2DM 为 1244±44ms,对照组为 1273±44ms,p=0.045)。
即使没有动脉高血压和显著 CAD,控制良好的 T2DM 患者在腺苷血管扩张应激时也表现出非对比 T1 最大反应减弱,这可能反映了冠状动脉微血管功能障碍。腺苷应激和静息 T1 映射可检测冠状动脉微血管的亚临床异常,而无需使用钆对比剂。CMR 可能在 T2DM 患者中识别出糖尿病心脏表型的早期特征和亚临床心脏风险标志物,为早期治疗干预提供机会。