Institute for Experimental and Translational Cardiovascular Imaging, University Hospital Frankfurt, Theodor-Stern Kai 7, 60590, Frankfurt am Main, Germany.
Department of Biomedical Sciences and Morphological and Functional Imaging, G. Martino University Hospital Messina, Via Consolare Valeria 1, Messina, 98100, Italy.
J Cardiovasc Magn Reson. 2020 Feb 6;22(1):14. doi: 10.1186/s12968-020-0600-1.
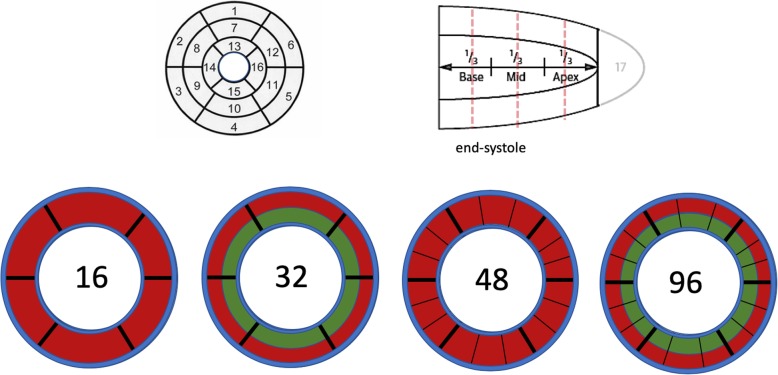
Myocardial perfusion with cardiovascular magnetic resonance (CMR) imaging is an established diagnostic test for evaluation of myocardial ischaemia. For quantification purposes, the 16 segment American Heart Association (AHA) model poses limitations in terms of extracting relevant information on the extent/severity of ischaemia as perfusion deficits will not always fall within an individual segment, which reduces its diagnostic value, and makes an accurate assessment of outcome data or a result comparison across various studies difficult. We hypothesised that division of the myocardial segments into epi- and endocardial layers and a further circumferential subdivision, resulting in a total of 96 segments, would improve the accuracy of detecting myocardial hypoperfusion. Higher (sub-)subsegmental recording of perfusion abnormalities, which are defined relatively to the normal reference using the subsegment with the highest value, may improve the spatial encoding of myocardial blood flow, based on a single stress perfusion acquisition.
A proof of concept comparison study of subsegmentation approaches based on transmural segments (16 AHA and 48 segments) vs. subdivision into epi- and endocardial (32) subsegments vs. further circumferential subdivision into 96 (sub-)subsegments for diagnostic accuracy against invasively defined obstructive coronary artery disease (CAD).
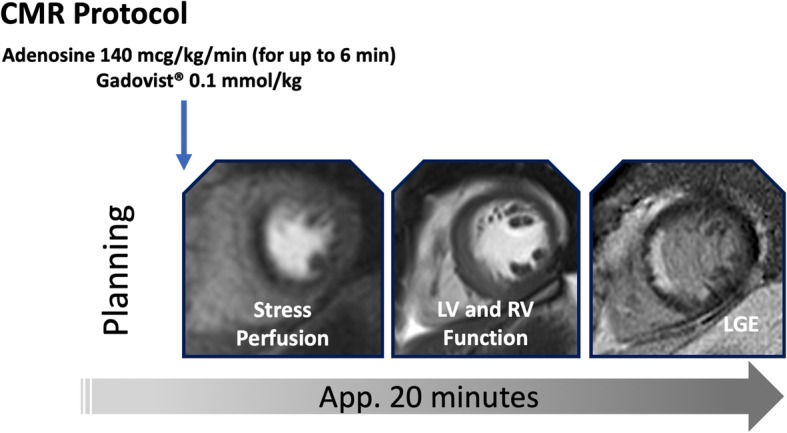
Thirty patients with obstructive CAD and 20 healthy controls underwent perfusion stress CMR imaging at 3 T during maximal adenosine vasodilation and a dual bolus injection of 0.1 mmol/kg gadobutrol. Using Fermi deconvolution for blood flow estimation, (sub-)subsegmental values were expressed relative to the (sub-)subsegment with the highest flow. In addition, endo-/epicardial flow ratios were calculated based on 32 and 96 (sub-)subsegments. A receiver operating characteristics (ROC) curve analysis was performed to compare the diagnostic performance of discrimination between patients with CAD and healthy controls. Observer reproducibility was assessed using Bland-Altman approaches.
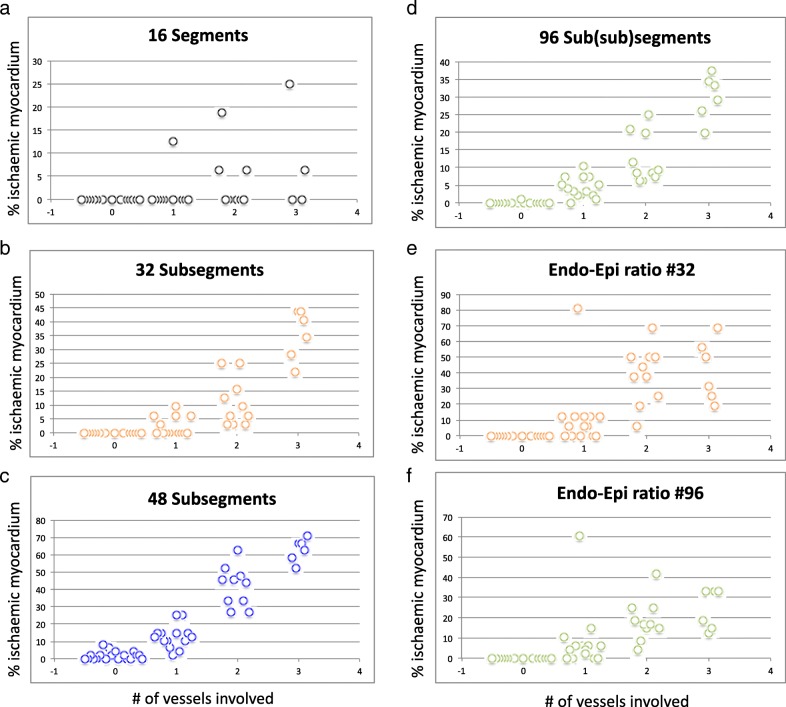
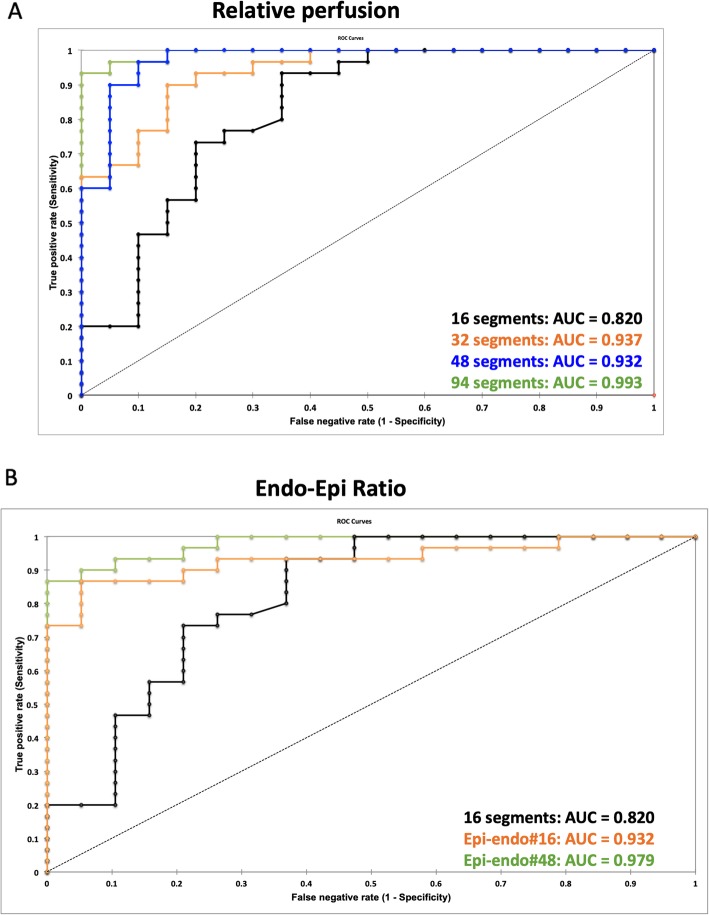
Subdivision into more and smaller segments revealed greater accuracy for #32, #48 and # 96 compared to the standard #16 approach (area under the curve (AUC): 0.937, 0.973 and 0.993 vs 0.820, p < 0.05). The #96-based endo-/epicardial ratio was superior to the #32 endo-/epicardial ratio (AUC 0.979, vs. 0.932, p < 0.05). Measurements for the #16 model showed marginally better reproducibility compared to #32, #48 and #96 (mean difference ± standard deviation: 2.0 ± 3.6 vs. 2.3 ± 4.0 vs 2.5 ± 4.4 vs. 4.1 ± 5.6).
Subsegmentation of the myocardium improves diagnostic accuracy and facilitates an objective cut-off-based description of hypoperfusion, and facilitates an objective description of hypoperfusion, including the extent and severity of myocardial ischaemia. Quantification based on a single (stress-only) pass reduces the overall amount of gadolinium contrast agent required and the length of the overall diagnostic study.
心血管磁共振(CMR)心肌灌注成像已成为评估心肌缺血的既定诊断测试。出于定量目的,美国心脏协会(AHA)的 16 节段模型在提取关于缺血程度/严重程度的相关信息方面存在局限性,因为灌注缺损并不总是位于单个节段内,这降低了其诊断价值,并使得对结果数据进行准确评估或在不同研究之间进行结果比较变得困难。我们假设将心肌节段划分为心外膜和心内膜层,并进一步进行圆周细分,总共产生 96 个节段,将提高检测心肌低灌注的准确性。较高的(亚)节段灌注异常记录,相对于使用具有最高值的亚节段定义为相对正常参考值,可能会基于单次应激灌注采集提高心肌血流的空间编码。
基于透壁节段(16 个 AHA 和 48 个节段)与心外膜和心内膜(32 个)细分与进一步圆周细分成 96 个(亚)节段(32 个)的亚节段方法的概念验证比较研究,以针对侵入性定义的阻塞性冠状动脉疾病(CAD)的诊断准确性。
30 例阻塞性 CAD 患者和 20 例健康对照者在 3T 下接受最大腺苷血管扩张和 0.1mmol/kg 钆布醇双重团注的应激 CMR 成像。使用费米反卷积法进行血流估计,(亚)节段值相对于具有最高血流的(亚)节段表示。此外,还基于 32 和 96 个(亚)节段计算了心外膜/心内膜的血流比值。进行了接收器操作特征(ROC)曲线分析,以比较区分 CAD 患者和健康对照者的诊断性能。使用 Bland-Altman 方法评估观察者的可重复性。
与标准的 16 节段方法相比,更多和更小的细分节段显示出更高的准确性(#32、#48 和#96 的曲线下面积(AUC)分别为 0.937、0.973 和 0.993 与 0.820,p < 0.05)。基于#96 的心外膜/心内膜比值优于基于#32 的心外膜/心内膜比值(AUC 0.979,vs. 0.932,p < 0.05)。与#32、#48 和#96 相比,#16 模型的测量值显示出略好的可重复性(平均差异 ± 标准差:2.0 ± 3.6 与 2.3 ± 4.0 与 2.5 ± 4.4 与 4.1 ± 5.6)。
心肌细分提高了诊断准确性,并有助于客观地描述低灌注,包括心肌缺血的程度和严重程度。基于单次(仅应激)通过的定量减少了所需的总体钆造影剂量和整体诊断研究的长度。