Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC.
Boston University School of Public Health, 715 Albany Street, Boston.
Medicine (Baltimore). 2021 Mar 26;100(12):e25231. doi: 10.1097/MD.0000000000025231.
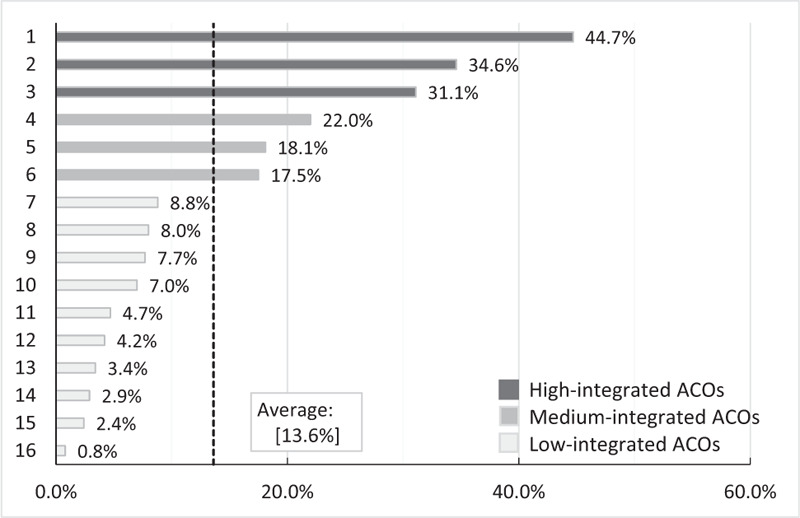
Physician-hospital integration among accountable care organizations (ACOs) has raised concern over impacts on prices and spending. However, characteristics of ACOs with greater integration between physicians and hospitals are unknown. We examined whether ACOs systematically differ by physician-hospital integration among 16 commercial ACOs operating in Massachusetts.Using claims data linked to information on physician affiliation, we measured hospital integration with primary care physicians for each ACO and categorized them into high-, medium-, and low-integrated ACOs. We conducted cross-sectional descriptive analysis to compare differences in patient population, organizational characteristics, and healthcare spending between the three groups. In addition, using multivariate generalized linear models, we compared ACO spending by integration level, adjusting for organization and patient characteristics. We identified non-elderly adults (aged 18-64) served by 16 Massachusetts ACOs over the period 2009 to 2013.High- and medium-integrated ACOs were more likely to be an integrated delivery system or an organization with a large number of providers. Compared to low-integrated ACOs, higher-integrated ACOs had larger inpatient care capacity, smaller composition of primary care physicians, and were more likely to employ physicians directly or through an affiliated hospital or physician group. A greater proportion of high-/medium-integrated ACO patients lived in affluent neighborhoods or areas with a larger minority population. Healthcare spending per enrollee in high-integrated ACOs was higher, which was mainly driven by a higher spending on outpatient facility services.This study shows that higher-integrated ACOs differ from their counterparts with low integration in many respects including higher healthcare spending, which persisted after adjusting for organizational characteristics and patient mix. Further investigation into the effects of integration on expenditures will inform the ongoing development of ACOs.
医疗机构整合型医疗照护组织(ACO)引起了人们对其对价格和支出影响的关注。然而,医师与医院整合程度较高的 ACO 特征尚不清楚。我们研究了在马萨诸塞州运营的 16 个商业 ACO 中,医师与医院整合程度不同的 ACO 是否存在系统性差异。
我们使用与医师从属关系信息相关联的索赔数据,衡量了每个 ACO 与初级保健医师的医院整合程度,并将其分为高、中、低整合 ACO。我们进行了横断面描述性分析,比较了三组之间的患者人群、组织特征和医疗保健支出差异。此外,我们使用多元广义线性模型,根据组织和患者特征调整了整合水平的 ACO 支出。
我们确定了在 2009 年至 2013 年期间由 16 个马萨诸塞州 ACO 服务的非老年成年人(18-64 岁)。高整合和中整合 ACO 更可能是综合交付系统或拥有大量提供者的组织。与低整合 ACO 相比,高整合 ACO 的住院治疗能力更大,初级保健医师的构成更小,并且更有可能通过附属医院或医师集团直接雇用医师。高/中整合 ACO 的患者中,有更大比例居住在富裕社区或少数民族人口较多的地区。高整合 ACO 每位参保人的医疗保健支出较高,这主要是由于门诊服务设施支出较高所致。
这项研究表明,在许多方面,高整合 ACO 与其低整合的同行存在差异,包括更高的医疗保健支出,这在调整了组织特征和患者构成后仍然存在。进一步研究整合对支出的影响将为 ACO 的持续发展提供信息。