Department of Emergency Medicine, University of Pennsylvania, Philadelphia.
Leonard Davis Institute of Health Economics, University of Pennsylvania, Philadelphia.
JAMA Netw Open. 2021 Mar 1;4(3):e213243. doi: 10.1001/jamanetworkopen.2021.3243.
Surgeons must balance management of acute postoperative pain with opioid stewardship. Patient-centered methods that immediately evaluate pain and opioid consumption can be used to guide prescribing and shared decision-making.
To assess the difference between the number of opioid tablets prescribed and the self-reported number of tablets taken as well as self-reported pain intensity and ability to manage pain after orthopedic and urologic procedures with use of an automated text messaging system.
DESIGN, SETTING, AND PARTICIPANTS: This quality improvement study was conducted at a large, urban academic health care system in Pennsylvania. Adult patients (aged ≥18 years) who underwent orthopedic and urologic procedures and received postoperative prescriptions for opioids were included. Data were collected prospectively using automated text messaging until postoperative day 28, from May 1 to December 31, 2019.
The primary outcome was the difference between the number of opioid tablets prescribed and the patient-reported number of tablets taken (in oxycodone 5-mg tablet equivalents). Secondary outcomes were self-reported pain intensity (on a scale of 0-10, with 10 being the highest level of pain) and ability to manage pain (on a scale of 0-10, with 10 representing very able to control pain) after orthopedic and urologic procedures.
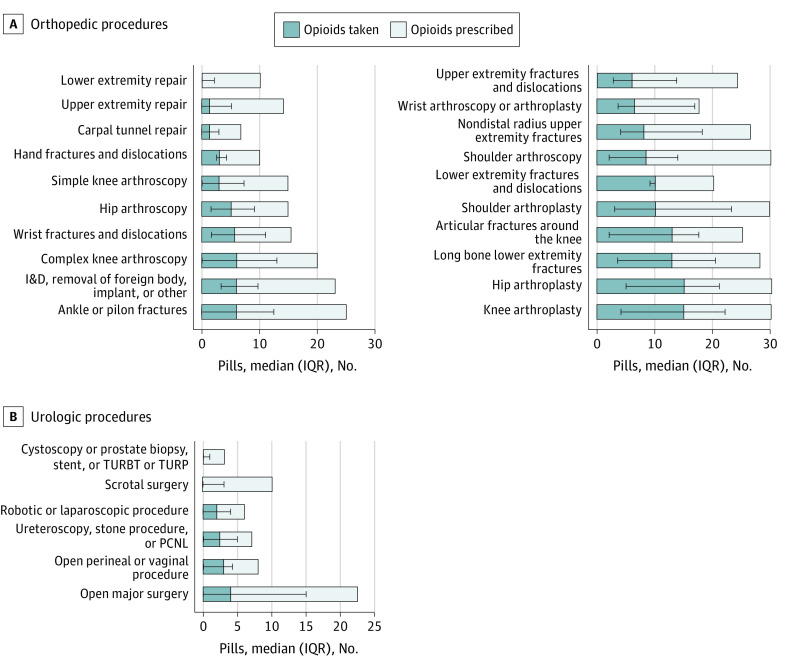
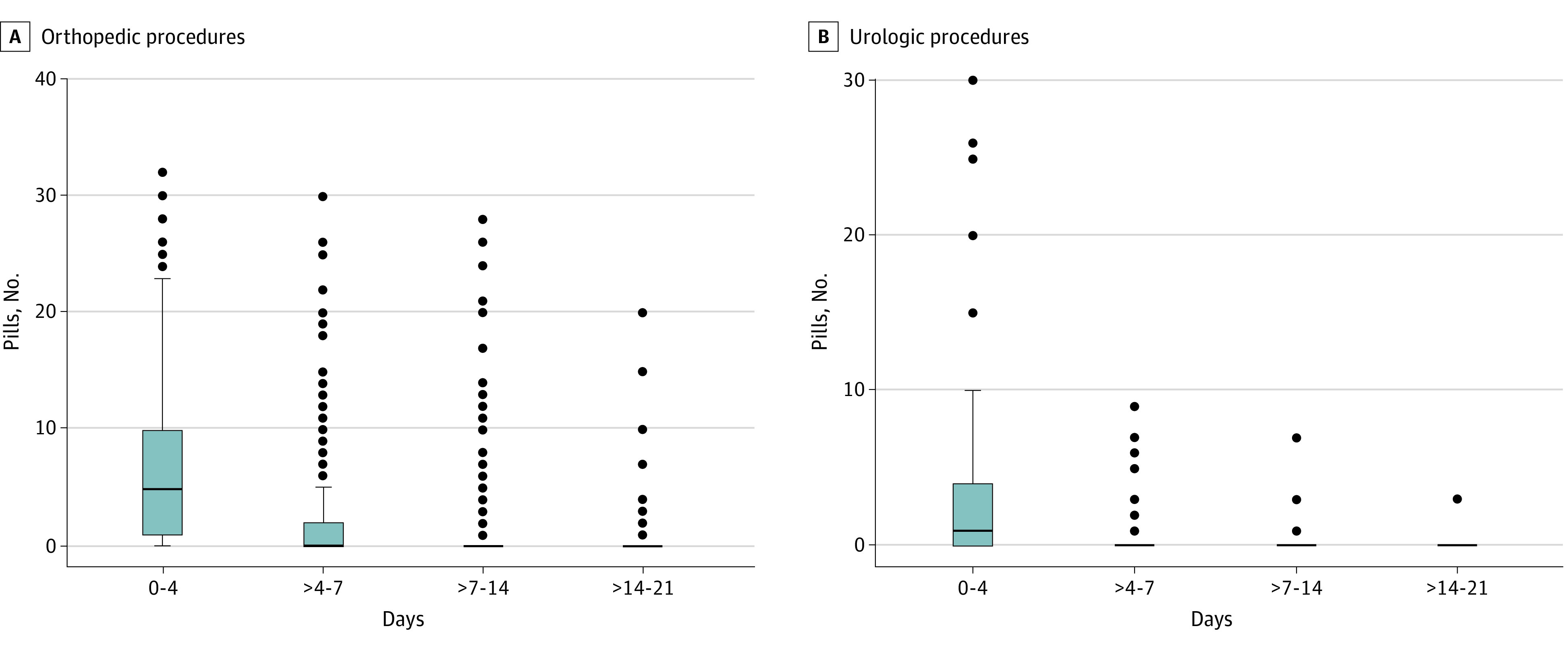
Of the 919 study participants, 742 (80.7%) underwent orthopedic procedures and 177 (19.2%) underwent urologic procedures. Among those who underwent orthopedic procedures, 384 (51.8%) were women, 491 (66.7%) were White, and the median age was 48 years (interquartile range [IQR], 32-61 years); 514 (69.8%) had an outpatient procedure. Among those who underwent urologic procedures, 145 (84.8%) were men, 138 (80.7%) were White, and the median age was 56 years (IQR, 40-67 years); 106 (62%) had an outpatient procedure. The mean (SD) pain score on day 4 after orthopedic procedures was 4.72 (2.54), with a mean (SD) change by day 21 of -0.40 (1.91). The mean (SD) ability to manage pain score on day 4 was 7.32 (2.59), with a mean (SD) change of -0.80 (2.72) by day 21. The mean (SD) pain score on day 4 after urologic procedures was 3.48 (2.43), with a mean (SD) change by day 21 of -1.50 (2.12). The mean (SD) ability to manage pain score on day 4 was 7.34 (2.81), with a mean (SD) change of 0.80 (1.75) by day 14. The median quantity of opioids prescribed for patients who underwent orthopedic procedures was high compared with self-reported consumption (20 tablets [IQR, 15-30 tablets] vs 6 tablets used [IQR, 0-14 tablets]), similar to findings for patients who underwent urologic procedures (7 tablets [IQR, 5-10 tablets] vs 1 tablet used [IQR, 0-4 tablets]). Over the study period, 9452 of 15 581 total tablets prescribed (60.7%) were unused. A total of 589 patients (64.1%) used less than half of the amount prescribed, and 256 patients (27.8%) did not use any opioids (179 [24.1%] who underwent orthopedic procedures and 77 [43.5%] who underwent urologic procedures).
In this quality improvement study of adult patients reporting use of opioids after common orthopedic and urologic surgical procedures through a text messaging system, the quantities of opioids prescribed and the quantity consumed differed. Patient-reported data collected through text messaging may support clinicians in tailoring prescriptions and guide shared decision-making to limit excess quantities of prescribed opioids.
重要性:外科医生必须在管理急性术后疼痛和阿片类药物管理之间取得平衡。以患者为中心的方法,可立即评估疼痛和阿片类药物的使用情况,有助于指导处方和共同决策。
目的:通过自动短信系统评估骨科和泌尿科手术后阿片类药物的处方片数与患者报告的服药片数以及自我报告的疼痛强度和管理疼痛能力之间的差异。
设计、设置和参与者:这项质量改进研究在宾夕法尼亚州一个大型城市学术医疗保健系统进行。纳入接受术后阿片类药物处方的接受骨科和泌尿科手术的成年患者(年龄≥18 岁)。从 2019 年 5 月 1 日至 12 月 31 日,前瞻性地使用自动短信收集数据,直到术后第 28 天。
主要结果和措施:主要结局是处方的阿片类药物片数与患者报告的服药片数(以羟考酮 5mg 片剂当量计)之间的差异。次要结局是骨科和泌尿科手术后自我报告的疼痛强度(0-10 分,10 分为最高疼痛水平)和管理疼痛的能力(0-10 分,10 分为非常能够控制疼痛)。
结果:在 919 名研究参与者中,742 名(80.7%)接受了骨科手术,177 名(19.2%)接受了泌尿科手术。在接受骨科手术的患者中,384 名(51.8%)为女性,491 名(66.7%)为白人,中位年龄为 48 岁(四分位距[IQR],32-61 岁);514 名(69.8%)为门诊手术。在接受泌尿科手术的患者中,145 名(84.8%)为男性,138 名(80.7%)为白人,中位年龄为 56 岁(IQR,40-67 岁);106 名(62%)为门诊手术。骨科手术后第 4 天的平均(SD)疼痛评分为 4.72(2.54),第 21 天的平均(SD)变化为-0.40(1.91)。第 4 天的平均(SD)疼痛管理能力评分为 7.32(2.59),第 21 天的平均(SD)变化为-0.80(2.72)。泌尿科手术后第 4 天的平均(SD)疼痛评分(3.48,2.43),第 21 天的平均(SD)变化为-1.50(2.12)。第 4 天的平均(SD)疼痛管理能力评分为 7.34(2.81),第 14 天的平均(SD)变化为 0.80(1.75)。与自我报告的使用量相比,接受骨科手术患者的阿片类药物处方量中位数较高(20 片[IQR,15-30 片]与 6 片使用[IQR,0-14 片]),与接受泌尿科手术患者的结果相似(7 片[IQR,5-10 片]与 1 片使用[IQR,0-4 片])。在研究期间,15581 片总处方中,9452 片(60.7%)未使用。共有 589 名患者(64.1%)使用了不到一半的处方量,256 名患者(27.8%)未使用任何阿片类药物(179 名接受骨科手术,77 名接受泌尿科手术)。
结论和相关性:在这项通过短信系统报告常见骨科和泌尿科手术后使用阿片类药物的成年患者的质量改进研究中,处方的阿片类药物数量和使用的数量不同。通过短信收集的患者报告数据可支持临床医生调整处方,并指导共同决策,以限制过量的处方阿片类药物。