Department of Ophthalmology and Visual Sciences, University of Maryland at Baltimore (UMB), Baltimore, Maryland, United States of America.
JHU Wilmer: Division of Neuro-Ophthalmology, Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland, United States of America.
PLoS One. 2021 Mar 25;16(3):e0243186. doi: 10.1371/journal.pone.0243186. eCollection 2021.
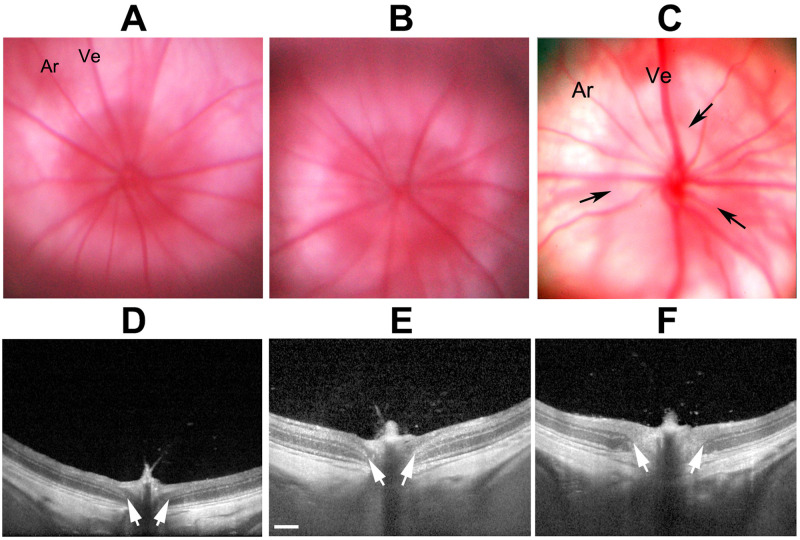
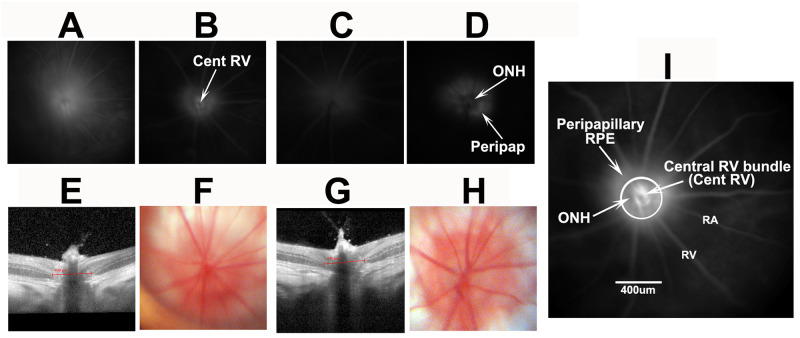
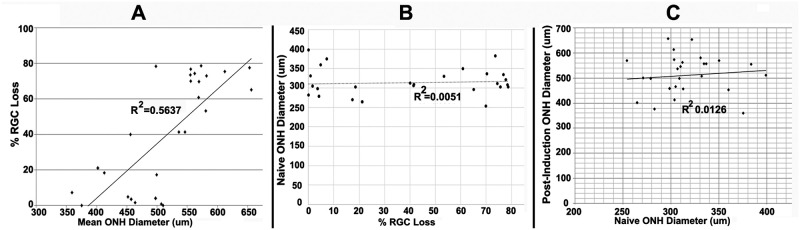
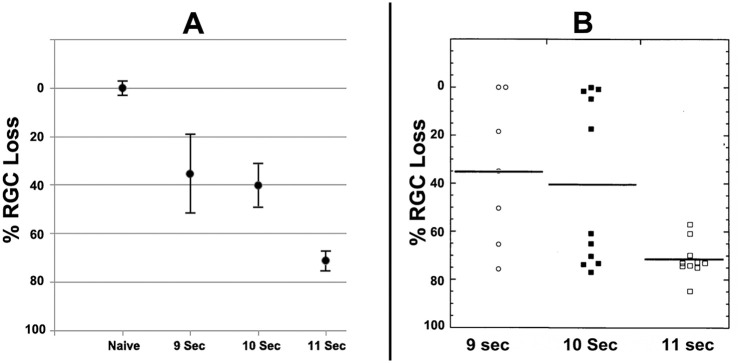
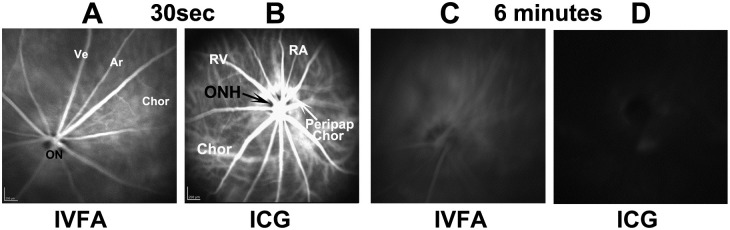
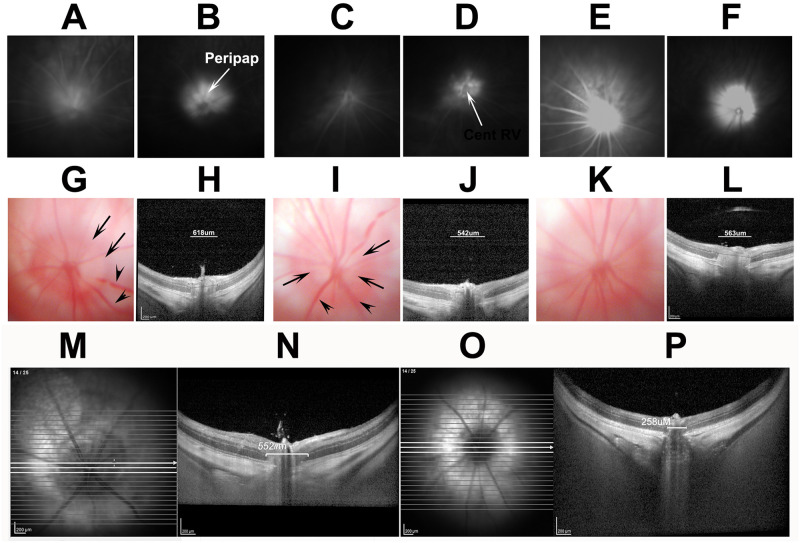
The rodent model of nonarteritic anterior ischemic optic neuropathy (rNAION) is similar in many of its pathophysiological responses to clinical NAION. Like human NAION, there is significant variability in the severity of the lesion produced, and little is known of the parameters associated with rNAION induction severity or if pre- or early post-induction biomarkers can be identified that enable prediction of lesion severity and ultimate loss of retinal ganglion cells (RGCs). Adult male Sprague-Dawley outbred rats were evaluated for various parameters including physiological characteristics (heart rate, respiratory rate, temperature, hematocrit [Hct]), optic nerve head (ONH) appearance, pre- and post-induction mean diameter, and intravenous fluorescein and indocyanine green angiographic patterns of vascular leakage at 5 hours post-induction, performed using a spectral domain-optical coherence tomography (SD-OCT) instrument. Early changes were correlated with ultimate RGC loss by Brn3a (+) immunohistology. RGC loss also was correlated with the relative level of laser exposure. The severity of ONH edema 2d, but not 5hr, post induction was most closely associated with the degree of RGC loss, revealing a threshold effect, and consistent with a compartment syndrome where a minimum level of capillary compression within a tight space is responsible for damage. RGC loss increased dramatically as the degree of laser exposure increased. Neither physiological parameters nor the degree of capillary leakage 5hr post induction were informative as to the ultimate degree of RGC loss. Similar to human NAION, the rNAION model exhibits marked variability in lesion severity. Unlike clinical NAION, pre-induction ONH diameter likely does not contribute to ultimate lesion severity; however, cross-sectional ONH edema can be used as a biomarker 2d post-induction to determine randomization of subjects prior to inclusion in specific neuroprotection or neuroregeneration studies.
非动脉炎性前部缺血性视神经病变(rNAION)的啮齿动物模型在许多病理生理反应方面与临床 NAION 相似。与人类 NAION 一样,病变的严重程度存在很大差异,而且对于与 rNAION 诱导严重程度相关的参数知之甚少,或者是否可以识别出诱导前或早期的生物标志物,从而能够预测病变严重程度和最终视网膜神经节细胞(RGC)的丧失。评估了成年雄性 Sprague-Dawley 远交大鼠的各种参数,包括生理特征(心率、呼吸频率、体温、红细胞压积[Hct])、视神经头(ONH)外观、诱导前和诱导后的平均直径,以及诱导后 5 小时的静脉内荧光素和吲哚菁绿血管渗漏的血管造影模式,使用光谱域光相干断层扫描(SD-OCT)仪器进行。早期变化与最终 RGC 丢失通过 Brn3a(+)免疫组织化学相关。RGC 丢失也与激光暴露的相对水平相关。诱导后 2d 的 ONH 水肿严重程度与 RGC 丢失的程度最密切相关,揭示了一个阈值效应,与间隙综合征一致,在这种综合征中,紧密空间内毛细血管的最小压缩程度负责损伤。随着激光暴露程度的增加,RGC 丢失急剧增加。诱导后 5 小时的生理参数或毛细血管渗漏程度均不能说明最终 RGC 丢失的程度。与人类 NAION 一样,rNAION 模型表现出病变严重程度的显著差异。与临床 NAION 不同,诱导前 ONH 直径可能不会导致最终病变严重程度;然而,诱导后 2d 的横截面 ONH 水肿可以用作生物标志物,以确定在将对象纳入特定的神经保护或神经再生研究之前进行随机分组。