McAllister Branduff, Gusella James F, Landwehrmeyer G Bernhard, Lee Jong-Min, MacDonald Marcy E, Orth Michael, Rosser Anne E, Williams Nigel M, Holmans Peter, Jones Lesley, Massey Thomas H
From the Division of Psychological Medicine and Clinical Neurosciences (B.M., N.M.W., P.H., L.J., T.H.M.), Brain Repair Group (A.E.R.), Schools of Medicine and Biosciences, and Neuroscience and Mental Health Research Institute (A.E.R.), Cardiff University, UK; Molecular Neurogenetic Unit (J.F.G., J.-M.L., M.E.M.), Center for Genomic Medicine, Massachusetts General Hospital; Department of Genetics (J.F.G., J.-M.L., M.E.M.), Harvard Medical School, Boston, MA; Department of Neurology (G.B.L.), University of Ulm, Germany; and Swiss Huntington's Disease Centre (M.O.), Siloah, Bern, Switzerland.
Neurology. 2021 May 11;96(19):e2395-e2406. doi: 10.1212/WNL.0000000000011893. Epub 2021 Mar 25.
To assess the prevalence, timing, and functional impact of psychiatric, cognitive, and motor abnormalities in Huntington disease (HD) gene carriers, we analyzed retrospective clinical data from individuals with manifest HD.
Clinical features of patients with HD were analyzed for 6,316 individuals in an observational study of the European Huntington's Disease Network (REGISTRY) from 161 sites across 17 countries. Data came from clinical history and the patient-completed Clinical Characteristics Questionnaire that assessed 8 symptoms: motor, cognitive, apathy, depression, perseverative/obsessive behavior, irritability, violent/aggressive behavior, and psychosis. Multiple logistic regression was used to analyze relationships between symptoms and functional outcomes.
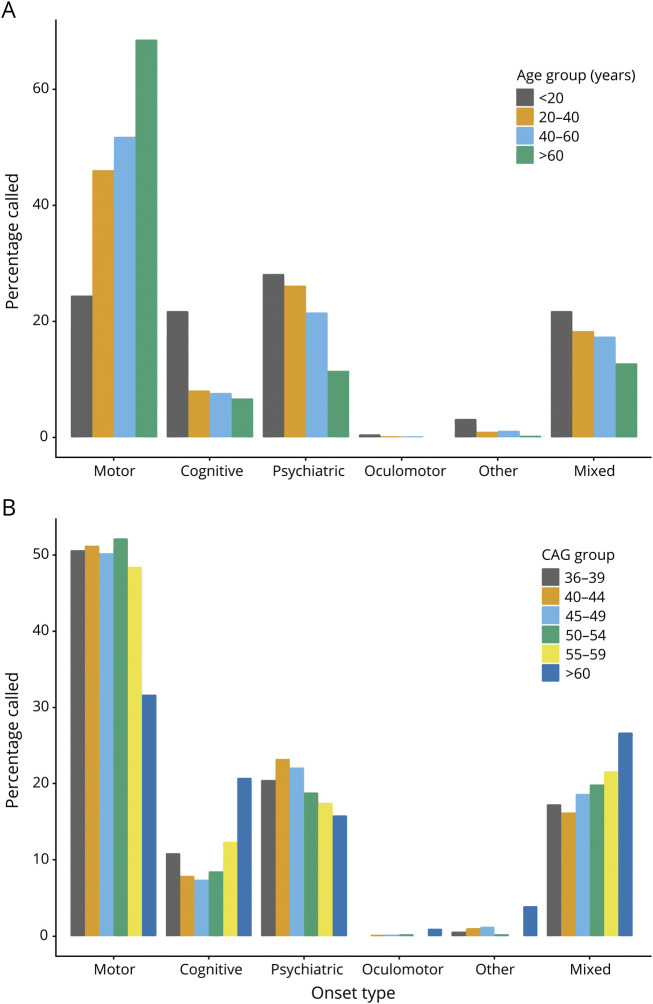
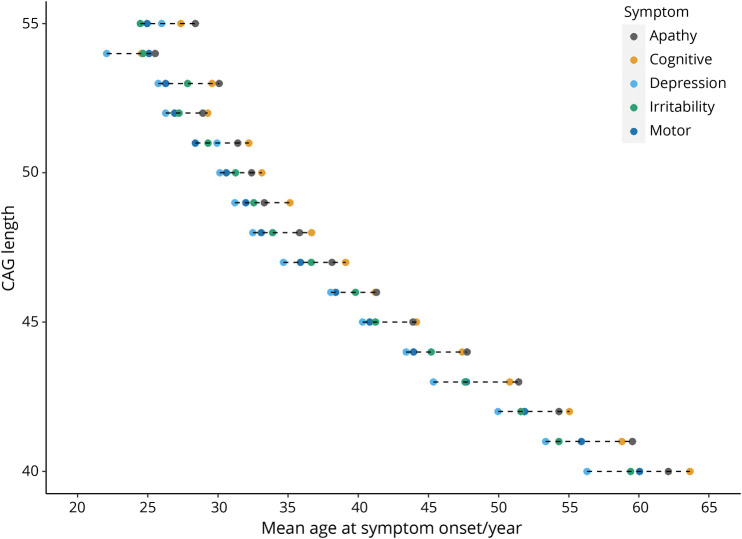
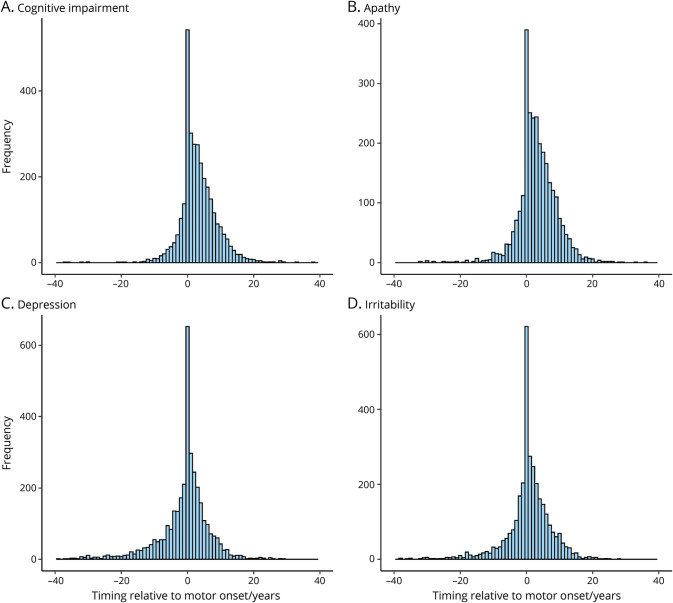
The initial manifestation of HD is increasingly likely to be motor and less likely to be psychiatric as age at presentation increases and is independent of pathogenic CAG repeat length. The Clinical Characteristics Questionnaire captures data on nonmotor symptom prevalence that correlate specifically with validated clinical measures. Psychiatric and cognitive symptoms are common in HD gene carriers, with earlier onsets associated with longer CAG repeats. Of patients with HD, 42.4% reported at least 1 psychiatric or cognitive symptom before motor symptoms, with depression most common. Each nonmotor symptom was associated with significantly reduced total functional capacity scores.
Psychiatric and cognitive symptoms are common and functionally debilitating in HD gene carriers. They require recognition and targeting with clinical outcome measures and treatments. However, because it is impossible to distinguish confidently between nonmotor symptoms arising from HD and primary psychiatric disorders, particularly in younger premanifest patients, nonmotor symptoms should not be used to make a clinical diagnosis of HD.
ClinicalTrials.gov Identifier: NCT01590589.
为评估亨廷顿舞蹈病(HD)基因携带者精神、认知和运动异常的患病率、出现时间及功能影响,我们分析了显性HD患者的回顾性临床数据。
在一项对欧洲亨廷顿舞蹈病网络(登记处)来自17个国家161个地点的6316名个体的观察性研究中,分析了HD患者的临床特征。数据来自临床病史以及患者填写的临床特征问卷,该问卷评估了8种症状:运动、认知、冷漠、抑郁、重复/强迫行为、易怒、暴力/攻击行为和精神病。采用多重逻辑回归分析症状与功能结局之间的关系。
随着发病年龄增加,HD的初始表现越来越可能是运动性的,而精神性的可能性越来越小,且与致病CAG重复长度无关。临床特征问卷收集了与经过验证的临床测量方法特异性相关的非运动症状患病率数据。精神和认知症状在HD基因携带者中很常见,发病较早与CAG重复较长有关。在HD患者中,42.4%报告在出现运动症状之前至少有1种精神或认知症状,其中抑郁最为常见。每种非运动症状都与总功能能力得分显著降低相关。
精神和认知症状在HD基因携带者中很常见且会导致功能衰退。它们需要通过临床结局测量和治疗来识别并针对性处理。然而,由于无法可靠地区分HD引起的非运动症状和原发性精神障碍,特别是在较年轻的症状前患者中,非运动症状不应被用于HD的临床诊断。
ClinicalTrials.gov标识符:NCT01590589。