Clarke Candice L, Prendecki Maria, Dhutia Amrita, Gan Jaslyn, Edwards Claire, Prout Virginia, Lightstone Liz, Parker Eleanor, Marchesin Federica, Griffith Megan, Charif Rawya, Pickard Graham, Cox Alison, McClure Myra, Tedder Richard, Randell Paul, Greathead Louise, Guckian Mary, McAdoo Stephen P, Kelleher Peter, Willicombe Michelle
Centre for Inflammatory Disease, Department of Immunology and Inflammation, Imperial College London, London, UK; Imperial College Renal and Transplant Centre, Division of Medicine, Imperial College Healthcare NHS Trust, Hammersmith Hospital, London, UK.
Centre for Inflammatory Disease, Department of Immunology and Inflammation, Imperial College London, London, UK; Imperial College Renal and Transplant Centre, Division of Medicine, Imperial College Healthcare NHS Trust, Hammersmith Hospital, London, UK.
Kidney Int. 2021 Jun;99(6):1470-1477. doi: 10.1016/j.kint.2021.03.009. Epub 2021 Mar 25.
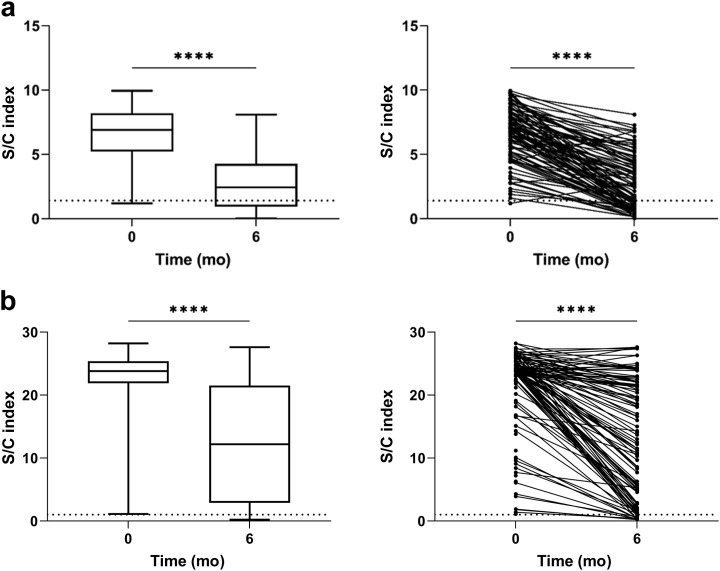
Patients with end stage kidney disease receiving in-center hemodialysis (ICHD) have had high rates of SARS-CoV-2 infection. Following infection, patients receiving ICHD frequently develop circulating antibodies to SARS-CoV-2, even with asymptomatic infection. Here, we investigated the durability and functionality of the immune responses to SARS-CoV-2 infection in patients receiving ICHD. Three hundred and fifty-six such patients were longitudinally screened for SARS-CoV-2 antibodies and underwent routine PCR-testing for symptomatic and asymptomatic infection. Patients were regularly screened for nucleocapsid protein (anti-NP) and receptor binding domain (anti-RBD) antibodies, and those who became seronegative at six months were screened for SARS-CoV-2 specific T-cell responses. One hundred and twenty-nine (36.2%) patients had detectable antibody to anti-NP at time zero, of whom 127 also had detectable anti-RBD. Significantly, at six months, 71/111 (64.0%) and 99/116 (85.3%) remained anti-NP and anti-RBD seropositive, respectively. For patients who retained antibody, both anti-NP and anti-RBD levels were reduced significantly after six months. Eleven patients who were anti-NP seropositive at time zero, had no detectable antibody at six months; of whom eight were found to have SARS-CoV-2 antigen specific T cell responses. Independent of antibody status at six months, patients with baseline positive SARS-CoV-2 serology were significantly less likely to have PCR confirmed infection over the following six months. Thus, patients receiving ICHD mount durable immune responses six months post SARS-CoV-2 infection, with fewer than 3% of patients showing no evidence of humoral or cellular immunity.
接受中心血液透析(ICHD)的终末期肾病患者感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)的比例很高。感染后,接受ICHD的患者即使无症状感染,也经常会产生针对SARS-CoV-2的循环抗体。在此,我们研究了接受ICHD的患者对SARS-CoV-2感染的免疫反应的持久性和功能。对356例此类患者进行了SARS-CoV-2抗体的纵向筛查,并对有症状和无症状感染进行了常规PCR检测。定期对患者进行核衣壳蛋白(抗NP)和受体结合域(抗RBD)抗体筛查,对6个月时血清学转为阴性的患者进行SARS-CoV-2特异性T细胞反应筛查。129例(36.2%)患者在零时可检测到抗NP抗体,其中127例也可检测到抗RBD抗体。值得注意的是,在6个月时,分别有71/111例(64.0%)和99/116例(85.3%)仍为抗NP和抗RBD血清阳性。对于保留抗体的患者,6个月后抗NP和抗RBD水平均显著降低。11例零时抗NP血清阳性的患者在6个月时未检测到抗体;其中8例被发现有SARS-CoV-2抗原特异性T细胞反应。无论6个月时的抗体状态如何,基线SARS-CoV-2血清学呈阳性的患者在接下来的6个月中PCR确诊感染的可能性显著降低。因此,接受ICHD的患者在感染SARS-CoV-2六个月后产生持久的免疫反应,不到3%的患者没有体液或细胞免疫的证据。