Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Division of Cardiology, Department of Medicine, Karolinska Institutet, Stockholm, Sweden.
Eur J Heart Fail. 2021 Jun;23(6):973-982. doi: 10.1002/ejhf.2169. Epub 2021 May 1.
We aimed to derive and validate clinically useful clusters of patients with heart failure with preserved ejection fraction (HFpEF; left ventricular ejection fraction ≥50%).
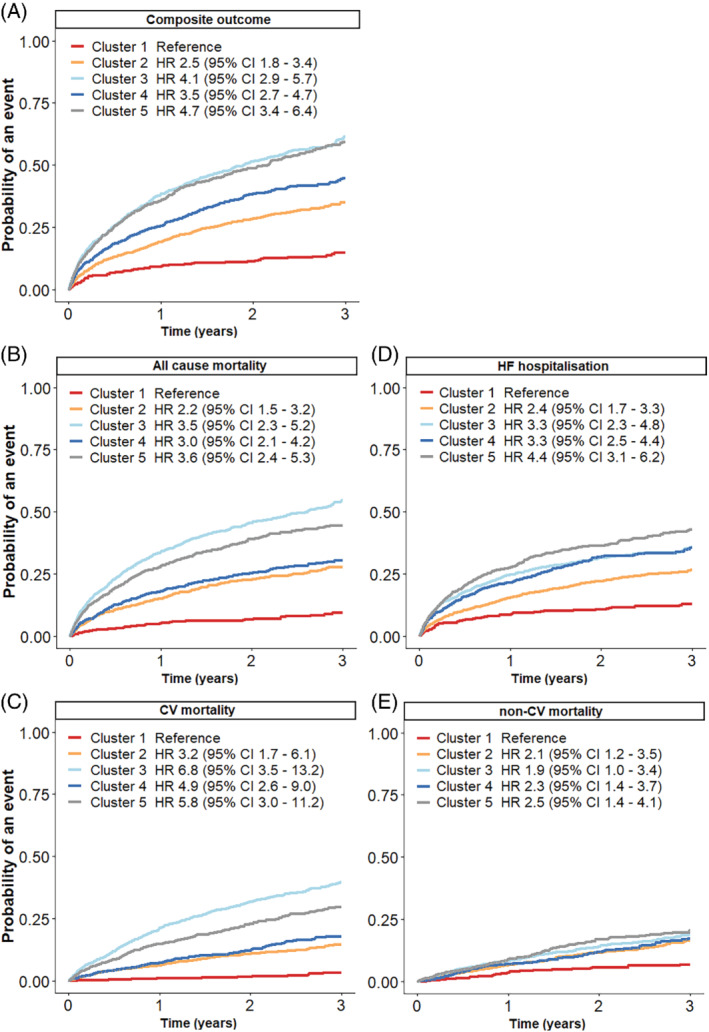
We derived a cluster model from 6909 HFpEF patients from the Swedish Heart Failure Registry (SwedeHF) and externally validated this in 2153 patients from the Chronic Heart Failure ESC-guideline based Cardiology practice Quality project (CHECK-HF) registry. In SwedeHF, the median age was 80 [interquartile range 72-86] years, 52% of patients were female and most frequent comorbidities were hypertension (82%), atrial fibrillation (68%), and ischaemic heart disease (48%). Latent class analysis identified five distinct clusters: cluster 1 (10% of patients) were young patients with a low comorbidity burden and the highest proportion of implantable devices; cluster 2 (30%) patients had atrial fibrillation, hypertension without diabetes; cluster 3 (25%) patients were the oldest with many cardiovascular comorbidities and hypertension; cluster 4 (15%) patients had obesity, diabetes and hypertension; and cluster 5 (20%) patients were older with ischaemic heart disease, hypertension and renal failure and were most frequently prescribed diuretics. The clusters were reproduced in the CHECK-HF cohort. Patients in cluster 1 had the best prognosis, while patients in clusters 3 and 5 had the worst age- and sex-adjusted prognosis.
Five distinct clusters of HFpEF patients were identified that differed in clinical characteristics, heart failure drug therapy and prognosis. These results confirm the heterogeneity of HFpEF and form a basis for tailoring trial design to individualized drug therapy in HFpEF patients.
我们旨在为射血分数保留的心力衰竭(HFpEF;左心室射血分数≥50%)患者推导并验证具有临床应用价值的聚类。
我们从瑞典心力衰竭注册(SwedeHF)中的 6909 例 HFpEF 患者中推导了一个聚类模型,并在慢性心力衰竭 ESC 指南为基础的心脏病实践质量项目(CHECK-HF)注册中的 2153 例患者中进行了外部验证。在 SwedeHF 中,中位年龄为 80 岁[四分位间距(IQR)72-86],52%的患者为女性,最常见的合并症为高血压(82%)、心房颤动(68%)和缺血性心脏病(48%)。潜在类别分析确定了五个不同的聚类:聚类 1(10%的患者)为年轻患者,合并症负担低,植入式设备比例最高;聚类 2(30%)患者患有心房颤动、无糖尿病的高血压;聚类 3(25%)患者年龄最大,心血管合并症多且患有高血压;聚类 4(15%)患者肥胖、患有糖尿病和高血压;聚类 5(20%)患者年龄较大,患有缺血性心脏病、高血压和肾衰竭,最常开利尿剂。这些聚类在 CHECK-HF 队列中得到重现。聚类 1 的患者预后最佳,而聚类 3 和聚类 5 的患者年龄和性别调整后预后最差。
确定了 5 种不同的 HFpEF 患者聚类,这些聚类在临床特征、心力衰竭药物治疗和预后方面存在差异。这些结果证实了 HFpEF 的异质性,并为针对 HFpEF 患者的个体化药物治疗量身定制试验设计奠定了基础。