Department of Cardiovascular Medicine, Nara Medical University, Kashihara, Japan.
Department of Cardiovascular Medicine, Hokkaido University Graduate School of Medicine, Sapporo, Japan.
ESC Heart Fail. 2023 Jun;10(3):2019-2030. doi: 10.1002/ehf2.14368. Epub 2023 Apr 12.
Heart failure (HF) with preserved ejection fraction (HFpEF) is a complex syndrome with a poor prognosis. Phenotyping is required to identify subtype-dependent treatment strategies. Phenotypes of Japanese HFpEF patients are not fully elucidated, whose obesity is much less than Western patients. This study aimed to reveal model-based phenomapping using unsupervised machine learning (ML) for HFpEF in Japanese patients.
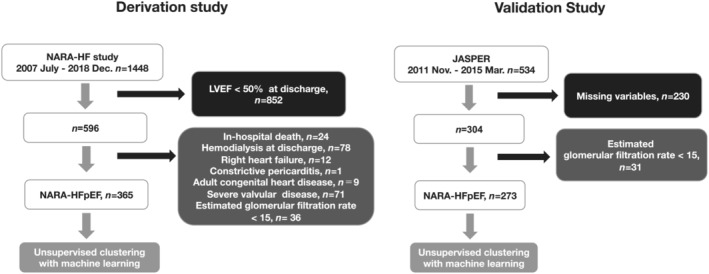
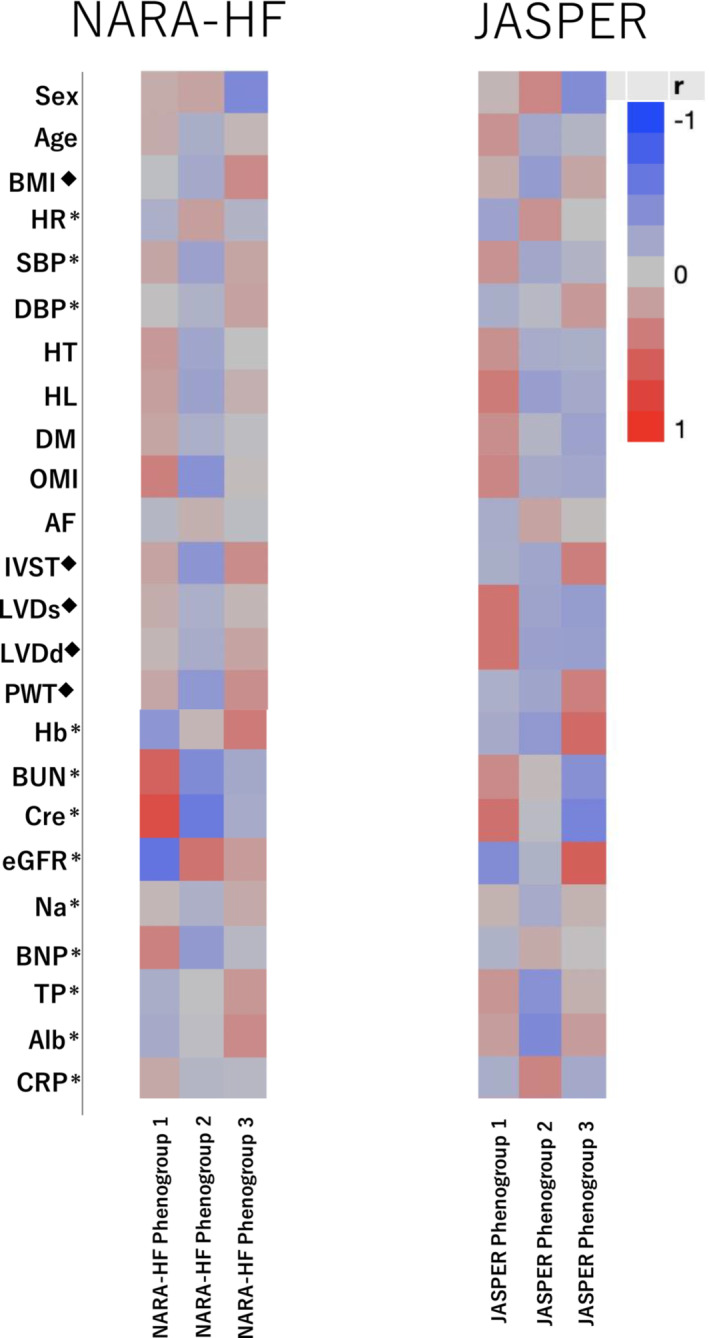
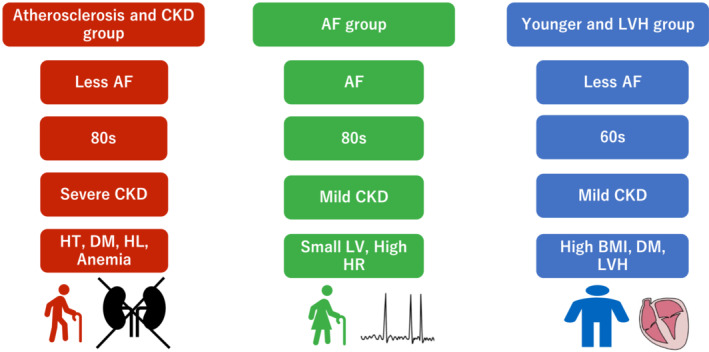
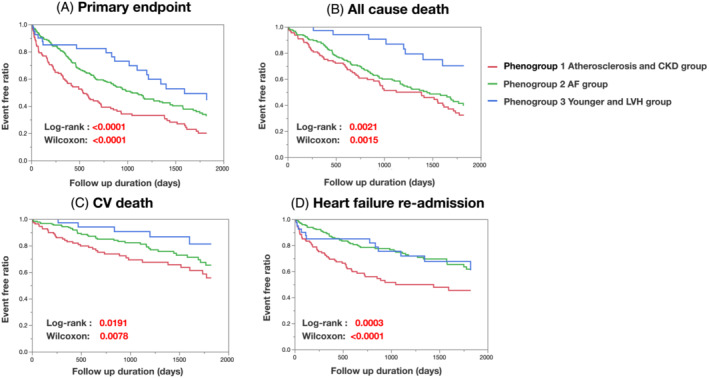
We studied 365 patients with HFpEF (left ventricular ejection fraction >50%) as a derivation cohort from the Nara Registry and Analyses for Heart Failure (NARA-HF), which registered patients with hospitalization by acute decompensated HF. We used unsupervised ML with a variational Bayesian-Gaussian mixture model (VBGMM) with common clinical variables. We also performed hierarchical clustering on the derivation cohort. We adopted 230 patients in the Japanese Heart Failure Syndrome with Preserved Ejection Fraction Registry as the validation cohort for VBGMM. The primary endpoint was defined as all-cause death and HF readmission within 5 years. Supervised ML was performed on the composite cohort of derivation and validation. The optimal number of clusters was three because of the probable distribution of VBGMM and the minimum Bayesian information criterion, and we stratified HFpEF into three phenogroups. Phenogroup 1 (n = 125) was older (mean age 78.9 ± 9.1 years) and predominantly male (57.6%), with the worst kidney function (mean estimated glomerular filtration rate 28.5 ± 9.7 mL/min/1.73 m ) and a high incidence of atherosclerotic factor. Phenogroup 2 (n = 200) had older individuals (mean age 78.8 ± 9.7 years), the lowest body mass index (BMI; 22.78 ± 3.94), and the highest incidence of women (57.5%) and atrial fibrillation (56.5%). Phenogroup 3 (n = 40) was the youngest (mean age 63.5 ± 11.2) and predominantly male (63.5 ± 11.2), with the highest BMI (27.46 ± 5.85) and a high incidence of left ventricular hypertrophy. We characterized these three phenogroups as atherosclerosis and chronic kidney disease, atrial fibrillation, and younger and left ventricular hypertrophy groups, respectively. At the primary endpoint, Phenogroup 1 demonstrated the worst prognosis (Phenogroups 1-3: 72.0% vs. 58.5% vs. 45%, P = 0.0036). We also successfully classified a derivation cohort into three similar phenogroups using VBGMM. Hierarchical and supervised clustering successfully showed the reproducibility of the three phenogroups.
ML could successfully stratify Japanese HFpEF patients into three phenogroups (atherosclerosis and chronic kidney disease, atrial fibrillation, and younger and left ventricular hypertrophy groups).
射血分数保留的心力衰竭(HFpEF)是一种预后不良的复杂综合征。需要表型分析来确定基于亚型的治疗策略。日本 HFpEF 患者的表型尚未完全阐明,其肥胖程度远低于西方患者。本研究旨在使用无监督机器学习(ML)揭示日本 HFpEF 患者的基于模型的表型映射。
我们研究了来自奈良登记和心力衰竭分析(NARA-HF)的 365 名 HFpEF(左心室射血分数>50%)患者作为推导队列,该登记通过急性失代偿性心力衰竭住院的患者。我们使用带有常见临床变量的变分贝叶斯-高斯混合模型(VBGMM)进行无监督 ML。我们还对推导队列进行了层次聚类。我们采用日本心力衰竭综合征伴射血分数保留登记处的 230 名患者作为 VBGMM 的验证队列。主要终点定义为 5 年内全因死亡和 HF 再入院。在推导和验证的综合队列上进行了有监督 ML。由于 VBGMM 和最小贝叶斯信息准则的可能分布,最佳聚类数为 3,我们将 HFpEF 分为三个表型组。表型组 1(n=125)年龄较大(平均年龄 78.9±9.1 岁),主要为男性(57.6%),肾功能最差(平均估算肾小球滤过率 28.5±9.7mL/min/1.73m ),动脉粥样硬化因素发生率高。表型组 2(n=200)患者年龄较大(平均年龄 78.8±9.7 岁),BMI 最低(22.78±3.94),女性(57.5%)和心房颤动(56.5%)发生率最高。表型组 3(n=40)是最年轻的(平均年龄 63.5±11.2 岁),主要为男性(63.5±11.2 岁),BMI 最高(27.46±5.85),左心室肥厚发生率高。我们将这三个表型组分别定义为动脉粥样硬化和慢性肾脏病、心房颤动以及年轻和左心室肥厚组。在主要终点,表型组 1 表现出最差的预后(表型组 1-3:72.0% vs. 58.5% vs. 45%,P=0.0036)。我们还使用 VBGMM 成功地将推导队列分为三个类似的表型组。层次聚类和有监督聚类成功地显示了三个表型组的可重复性。
ML 可以成功地将日本 HFpEF 患者分为三个表型组(动脉粥样硬化和慢性肾脏病、心房颤动以及年轻和左心室肥厚组)。