Department of Radiology, Dresden University Hospital, Fetscherstr. 74, 01307, Dresden, Germany.
Department of Nuclear Medicine, Dresden University Hospital, Fetscherstr. 74, 01307, Dresden, Germany.
Abdom Radiol (NY). 2021 Aug;46(8):4046-4055. doi: 10.1007/s00261-021-03048-1. Epub 2021 Mar 29.
Preoperative hypertrophy induction of future liver remnant (FLR) reduces the risk of postoperative liver insufficiency after partial hepatectomy. One of the most commonly used methods to induce hypertrophy of FLR is portal vein embolization (PVE). Recent studies have shown that transarterial radioembolization (TARE) also induces hypertrophy of the contralateral liver lobe. The aim of our study was to evaluate contralateral hypertrophy after TARE versus after PVE taking into account the effect of cirrhosis.
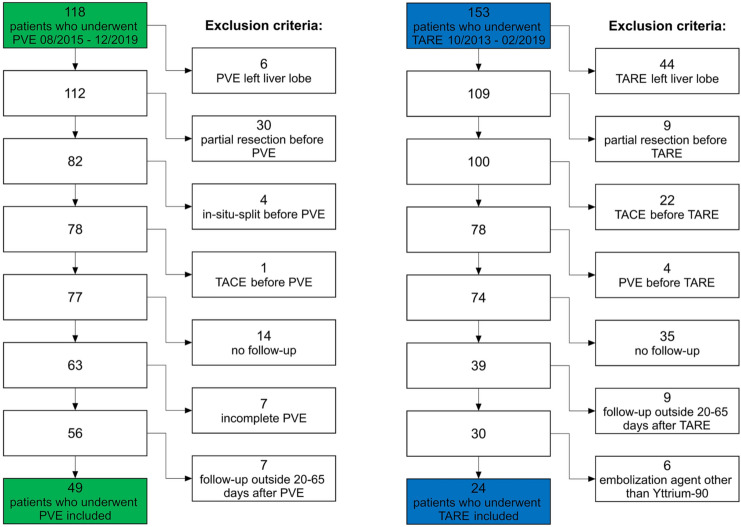
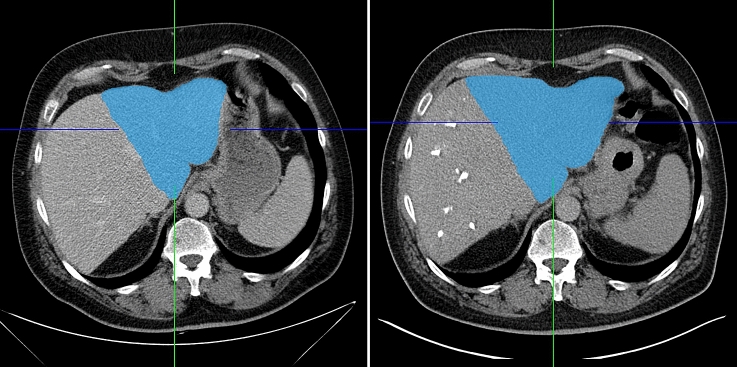
Forty-nine patients undergoing PVE before hemihepatectomy and 24 patients with TARE as palliative treatment for liver malignancy were retrospectively included. Semi-automated volumetry of the FLR/contralateral liver lobe before and after intervention (20 to 65 days) was performed on CT or MRI, and the relative increase in volume was calculated. Cirrhosis was evaluated independently by two radiologists on CT/MRI, and interrater reliability was calculated.
Hypertrophy after PVE was significantly more pronounced than after TARE (25.3% vs. 7.4%; p < 0.001). In the subgroup of patients without cirrhosis, the difference was also statistically significant (25.9% vs. 8.6%; p = 0.002), whereas in patients with cirrhosis, the difference was not statistically significant (18.2% vs. 7.4%; p = 0.212). After PVE, hypertrophy in patients without cirrhosis was more pronounced than in patients with cirrhosis (25.9% vs. 18.2%; p = 0.203), while after TARE, hypertrophy was comparable in patients with and without cirrhosis (7.4% vs. 8.6%; p = 0.928).
TARE induces less pronounced hypertrophy of the FLR compared to PVE. Cirrhosis seems to be less of a limiting factor for hypertrophy after TARE, compared to PVE.
术前诱导未来肝残肝(FLR)肥大可降低部分肝切除术后肝功能不全的风险。诱导 FLR 肥大最常用的方法之一是门静脉栓塞术(PVE)。最近的研究表明,经动脉放射性栓塞术(TARE)也可诱导对侧肝叶肥大。本研究旨在评估 TARE 与 PVE 后对侧肝叶肥大,同时考虑肝硬化的影响。
回顾性纳入 49 例行半肝切除术前行 PVE 及 24 例行 TARE 姑息性治疗肝脏恶性肿瘤的患者。在 CT 或 MRI 上对干预前后(20 至 65 天)的 FLR/对侧肝叶进行半自动容积测量,并计算体积的相对增加。肝硬化由两位放射科医生在 CT/MRI 上独立评估,并计算组内相关系数。
PVE 后肝肥大程度明显大于 TARE(25.3%比 7.4%;p<0.001)。在无肝硬化患者亚组中,差异也具有统计学意义(25.9%比 8.6%;p=0.002),而在肝硬化患者中,差异无统计学意义(18.2%比 7.4%;p=0.212)。PVE 后,无肝硬化患者的肝肥大程度明显大于肝硬化患者(25.9%比 18.2%;p=0.203),而 TARE 后,肝硬化与非肝硬化患者的肝肥大程度相似(7.4%比 8.6%;p=0.928)。
与 PVE 相比,TARE 诱导 FLR 肥大的程度较轻。与 PVE 相比,肝硬化对 TARE 后肝肥大的限制作用较小。