Böning Georg, Fehrenbach Uli, Auer Timo Alexander, Neumann Konrad, Jonczyk Martin, Pratschke Johann, Schöning Wenzel, Schmelzle Moritz, Gebauer Bernhard
Department of Radiology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Augustenburger Platz 1, 13353, Berlin, Germany.
Berlin Institute of Health (BIH), Anna-Louisa-Karsch-Straße 2, 10178, Berlin, Germany.
Cardiovasc Intervent Radiol. 2022 Jul;45(7):950-957. doi: 10.1007/s00270-022-03107-0. Epub 2022 Mar 21.
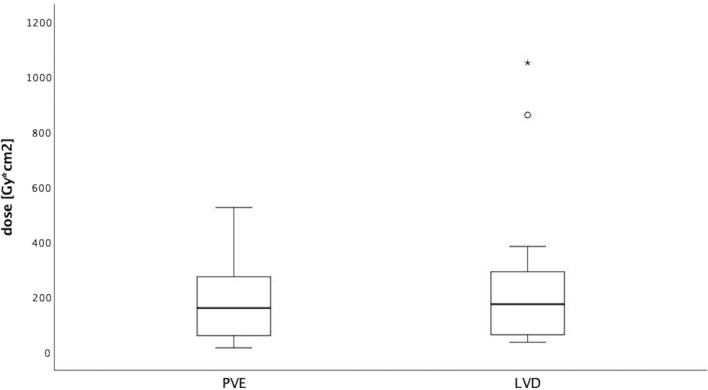
To investigate whether liver venous deprivation (LVD) as simultaneous, portal vein (PVE) and right hepatic vein embolization offers advantages in terms of hypertrophy induction before extended hepatectomy in non-cirrhotic liver.
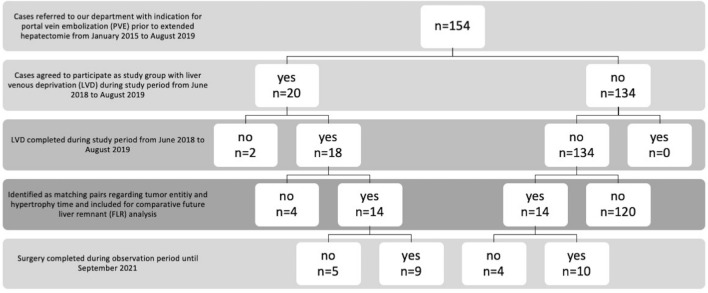
Between June 2018 and August 2019, 20 patients were recruited for a prospective, non-randomized study to investigate the efficacy of LVD. After screening of 134 patients treated using PVE alone from January 2015 to August 2019, 14 directly matched pairs regarding tumor entity (cholangiocarcinoma, CC and colorectal carcinoma, CRC) and hypertrophy time (defined as time from embolization to follow-up imaging) were identified. In both treatment groups, the same experienced reader (> 5 years experience) performed imaging-based measurement of the volumes of liver segments of the future liver remnant (FLR) prior to embolization and after the standard clinical hypertrophy interval (~ 30 days), before surgery. Percentage growth of segments was calculated and compared.
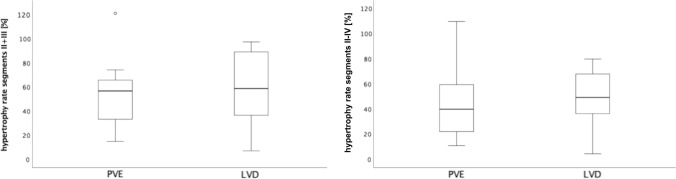
After matched follow-up periods (mean of 30.5 days), there were no statistically significant differences in relative hypertrophy of FLRs. Mean ± standard deviation relative hypertrophy rates for LVD/PVE were 59 ± 29.6%/54.1 ± 27.6% (p = 0.637) for segments II + III and 48.2 ± 22.2%/44.9 ± 28.9% (p = 0.719) for segments II-IV, respectively.
LVD had no significant advantages over the standard method (PVE alone) in terms of hypertrophy induction of the FLR before extended hepatectomy in this study population.
探讨在非肝硬化肝脏扩大肝切除术前,同时进行肝静脉剥夺(LVD)、门静脉栓塞(PVE)和右肝静脉栓塞在诱导肝肥大方面是否具有优势。
2018年6月至2019年8月,招募了20名患者进行一项前瞻性、非随机研究,以调查LVD的疗效。在筛选了2015年1月至2019年8月仅接受PVE治疗的134名患者后,确定了14对在肿瘤类型(胆管癌,CC和结直肠癌,CRC)和肥大时间(定义为从栓塞到随访成像的时间)方面直接匹配的患者。在两个治疗组中,由同一位经验丰富的阅片者(>5年经验)在栓塞前、标准临床肥大间隔(约30天)后、手术前,对未来肝残余(FLR)肝段的体积进行基于影像的测量。计算并比较各肝段的生长百分比。
在匹配的随访期(平均30.5天)后,FLR的相对肥大情况无统计学显著差异。LVD/PVE组中,II+III段的平均±标准差相对肥大率分别为59±29.6%/54.1±27.6%(p=0.637),II-IV段为48.2±22.2%/44.9±28.9%(p=0.719)。
在本研究人群中,在扩大肝切除术前诱导FLR肝肥大方面,LVD与标准方法(仅PVE)相比无显著优势。