Department of Surgery, Amsterdam UMC, University of Amsterdam, Cancer Center Amsterdam, Amsterdam, The Netherlands.
Cancer Center Amsterdam, Amsterdam, The Netherlands.
World J Surg. 2021 Aug;45(8):2463-2470. doi: 10.1007/s00268-021-06036-0. Epub 2021 Mar 30.
Open resection of small bowel neuroendocrine neoplasms (SB-NEN) is still considered standard-of-care, mainly because of frequently encountered multifocality and central mesenteric masses. The aim of this study was to evaluate surgical approach for SB-NEN at a national level and determine predictors for overall survival.
Patients with SB-NEN who underwent resection between 2005 and 2015 were included from the Netherlands Cancer Registry. Patient and tumor characteristics were compared between laparoscopic and open approach. Overall survival was assessed by Kaplan-Meier and compared with the Log-rank test. Independent predictors were determined by Cox proportional hazards model.
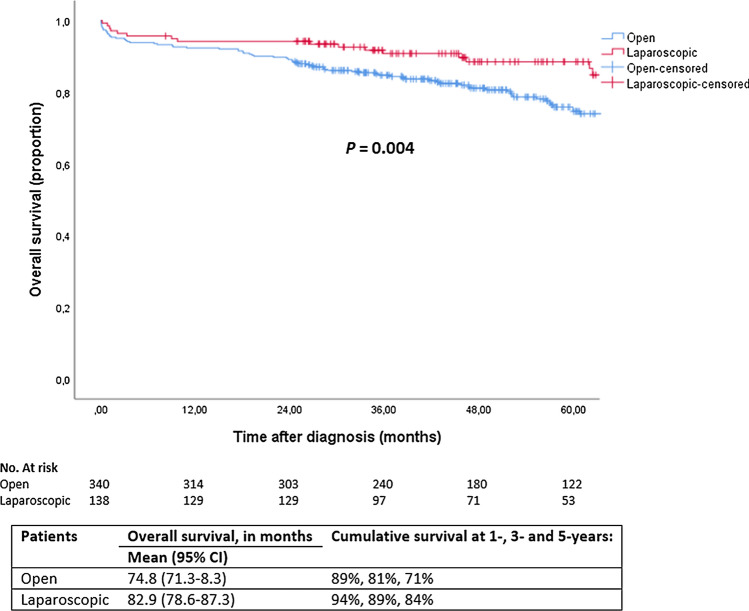
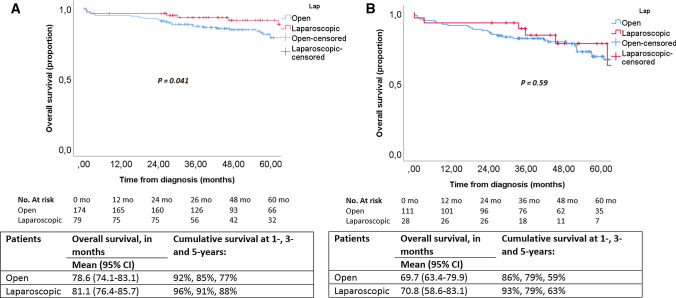
In total, 482 patients were included, of whom 342 (71%) underwent open and 140 (29%) laparoscopic resection. The open resection group had significantly more multifocal tumors resected (24% vs. 14%), pN2 lymph nodes (18% vs. 7%) and stage IV disease (36% vs. 22%). Overall survival after open resection was significantly shorter compared to laparoscopic resection (3-year: 81% vs. 89%, 5-year: 71% vs. 84%, p = 0.004). In multivariable analysis, age above 60-years (60-75, HR 3.38 (95% CI 1.84-6.23); > 75 years, HR 7.63 (95% CI 3.86-15.07)), stage IV disease (HR 1.86 (95% CI 1.18-2.94)) and a laparoscopic approach (HR 0.51 (95% CI 0.28-0.94)) were independently associated with overall survival, whereas multifocal primary tumor, grade and resection margin status were not.
Laparoscopic resection was the approach in 29% of SB-NEN at a national level with selection of the more favorable patients. Laparoscopic resection remained independently associated with better overall survival besides age and stage, but residual confounding cannot be excluded.
开腹手术切除小肠神经内分泌肿瘤(SB-NEN)仍然被认为是标准治疗方法,主要是因为常遇到多发病灶和中央肠系膜肿块。本研究旨在评估全国范围内 SB-NEN 的手术方法,并确定总生存率的预测因素。
从荷兰癌症登记处纳入 2005 年至 2015 年间接受 SB-NEN 切除术的患者。比较腹腔镜和开腹手术的患者和肿瘤特征。通过 Kaplan-Meier 评估总生存率,并通过对数秩检验进行比较。通过 Cox 比例风险模型确定独立预测因素。
共纳入 482 例患者,其中 342 例(71%)行开腹切除术,140 例(29%)行腹腔镜切除术。开腹组切除的多灶性肿瘤明显更多(24%比 14%),pN2 淋巴结(18%比 7%)和 IV 期疾病(36%比 22%)。开腹切除术后的总生存率明显短于腹腔镜切除术后(3 年:81%比 89%,5 年:71%比 84%,p=0.004)。多变量分析显示,年龄 60-75 岁(HR 3.38(95%CI 1.84-6.23); > 75 岁,HR 7.63(95%CI 3.86-15.07))、IV 期疾病(HR 1.86(95%CI 1.18-2.94))和腹腔镜方法(HR 0.51(95%CI 0.28-0.94))与总生存率独立相关,而多发病灶、分级和切缘状态则无关。
腹腔镜切除在全国范围内的 SB-NEN 中占 29%,选择了更有利的患者。除年龄和分期外,腹腔镜切除仍与更好的总生存率独立相关,但仍不能排除残留混杂因素。