Negoi Ionut, Hostiuc Sorin, Negoi Ruxandra Irina, Beuran Mircea
Department of General Surgery, Emergency Hospital of Bucharest, Carol Davila University of Medicine and Pharmacy Bucharest, Bucharest 014461, Romania.
National Institute of Legal Medicine Mina Minovici, Carol Davila University of Medicine and Pharmacy Bucharest, Bucharest 014461, Romania.
World J Gastrointest Oncol. 2017 Dec 15;9(12):475-491. doi: 10.4251/wjgo.v9.i12.475.
To compare the effectiveness of laparoscopic complete mesocolic excision (CME) with central vascular ligation (L-CME) with its open (O-CME) counterpart.
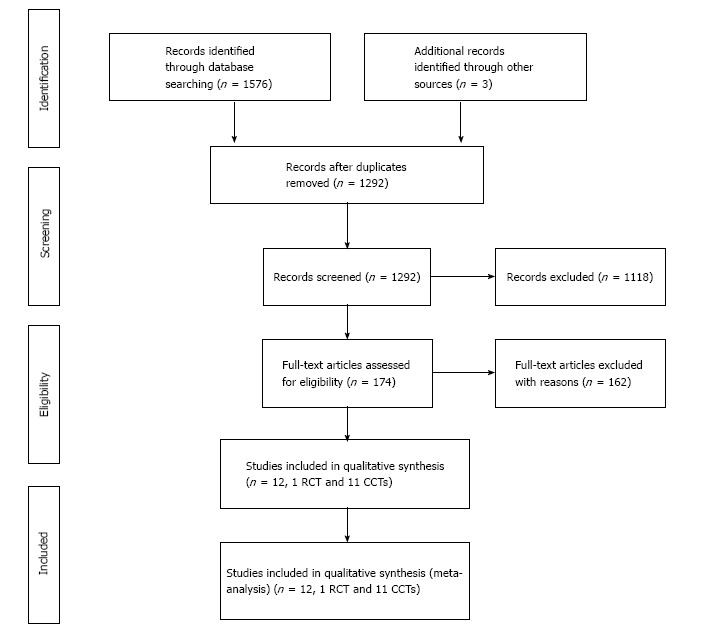
We conducted an electronic search of the PubMed/MEDLINE, Excerpta Medica Database, Web of Science Core Collection, Cochrane Center Register of Controlled Trails, Cochrane Database of Systematic Reviews, SciELO, and Korean Journal databases from their inception until May 2017. We considered randomized controlled trials (RCTs) and controlled clinical trials (CCTs) that included patients with colonic cancer comparing L-CME and O-CME. Primary outcomes included the quality of the resected specimen (lymph nodes retrieved, complete mesocolic plane excision, tumor to arterial high tie, resected mesocolon surface). Secondary outcomes included the three-year and five-year overall and disease-free survival rates, recurrence of the disease, surgical data, and postoperative morbidity and mortality. Two authors of the review screened the methodological quality of the eligible trials and independently extracted data from individual studies.
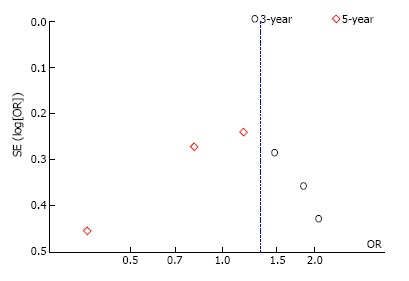
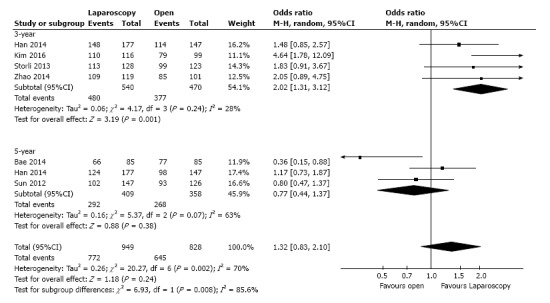
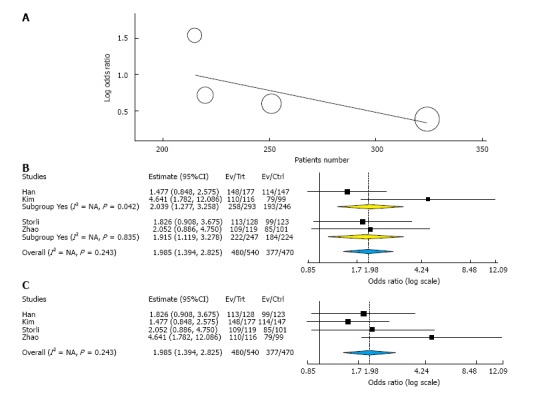
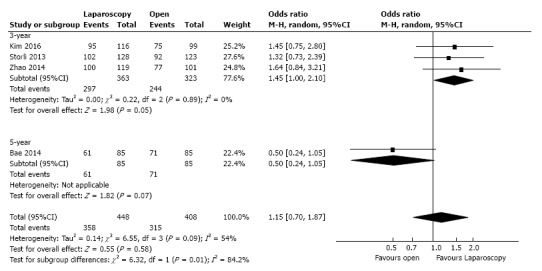
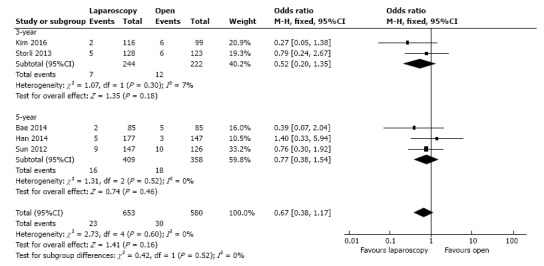
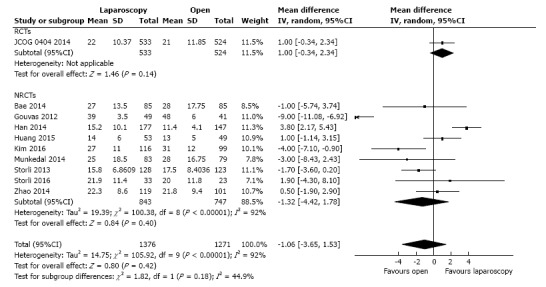
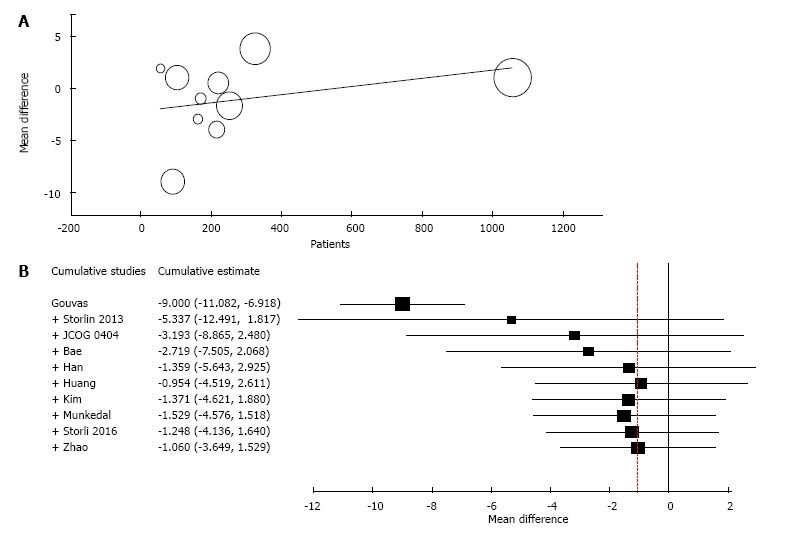
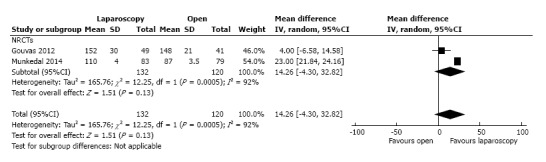
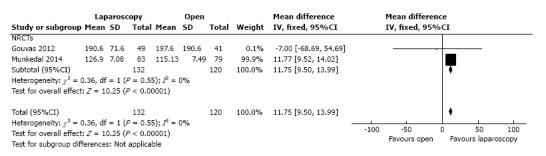
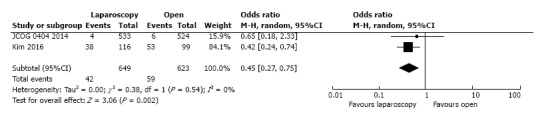
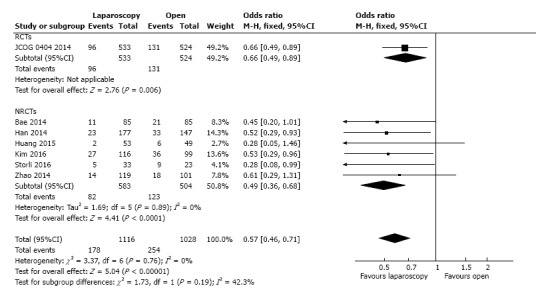
A total of one RCT and eleven CCTs (four from Europe and seven from Asia) met the inclusion criteria for the current meta-analysis. These studies involved 1619 patients in L-CME and 1477 patients in O-CME. The L-CME was associated with the same quality of the resected specimen, with no differences regarding the retrieved lymphnodes (MD = -1.06, 95%CI: -3.65 to 1.53, = 0.42), and tumor to high tie distance (MD = 14.26 cm, 95%CI: -4.30 to 32.82, = 0.13); the surface of the resected mesocolon was higher in the L-CME group (MD = 11.75 cm, 95%CI: 9.50 to 13.99, < 0.001). The L-CME was associated with a lower rate of blood transfusions (OR = 0.45, 95%CI: 0.27 to 0.75, = 0.002), faster recovery of gastrointestinal function, and less postoperative overall complication rate. The L-CME approach was associated with a statistical significant better three-year overall (OR = 2.02, 95%CI: 1.31 to 3.12, = 0.001, = 28%) and disease-free (OR = 1.45, 95% CI: 1.00 to 2.10, = 0.05, = 0%) survival.
The laparoscopic approach offers the same quality of the resected specimen as the open approach in complete mesocolic excision with central vascular ligation for colon cancer. The laparoscopic complete mesocolic excision with central vascular ligation is superior in all perioperative results and at least non-inferior in long-term oncological outcomes.
比较腹腔镜全结肠系膜切除术(CME)联合中央血管结扎术(L-CME)与开放手术(O-CME)的效果。
我们对PubMed/MEDLINE、医学文摘数据库、科学引文索引核心合集、Cochrane对照试验中心注册库、Cochrane系统评价数据库、SciELO以及韩国期刊数据库进行了电子检索,检索时间从各数据库建库至2017年5月。我们纳入了比较L-CME和O-CME的随机对照试验(RCT)和对照临床试验(CCT),这些试验的研究对象为结肠癌患者。主要结局包括切除标本的质量(获取的淋巴结数量、全结肠系膜平面切除情况、肿瘤至动脉高位结扎的距离、切除的结肠系膜表面)。次要结局包括三年和五年总生存率及无病生存率、疾病复发情况、手术数据以及术后发病率和死亡率。两位综述作者筛选了符合条件试验的方法学质量,并独立从各个研究中提取数据。
共有1项RCT和11项CCT(4项来自欧洲,7项来自亚洲)符合当前荟萃分析的纳入标准。这些研究中,L-CME组有1619例患者,O-CME组有1477例患者。L-CME组切除标本的质量相同,获取的淋巴结数量(MD = -1.06,95%CI:-3.65至1.53,P = 0.42)以及肿瘤至高位结扎距离(MD = 14.26 cm,95%CI:-4.30至32.82,P = 0.13)方面无差异;L-CME组切除的结肠系膜表面更高(MD = 11.75 cm,95%CI:9.50至13.99,P < 0.001)。L-CME组输血率较低(OR = 0.45,95%CI:0.27至0.75,P = 0.002),胃肠功能恢复更快,术后总体并发症发生率更低。L-CME手术方式在三年总生存率(OR = 2.02,95%CI:1.31至3.12,P = 0.001,I² = 28%)和无病生存率(OR = 1.45,95%CI:1.00至2.10,P = 0.05,I² = 0%)方面具有统计学意义的更好结果。
在结肠癌全结肠系膜切除联合中央血管结扎术中,腹腔镜手术方式与开放手术方式切除标本的质量相同。腹腔镜全结肠系膜切除联合中央血管结扎术在所有围手术期结果方面更优,且在长期肿瘤学结局方面至少不劣于开放手术。