Department of Anesthesiology, Renmin Hospital of Wuhan University, No. 99 Zhang Road, Wuhan, 430060, Hubei Province, China.
Department of Psychiatry, Renmin Hospital of Wuhan University, No. 99 Zhang Road, Wuhan, 430060, Hubei Province, China.
BMC Anesthesiol. 2021 Mar 31;21(1):98. doi: 10.1186/s12871-021-01291-z.
Ultrasound-guided parasternal intercostal nerve block is rarely used for postoperative analgesia, and its value remains unclear. This study aimed to evaluate the effectiveness of ultrasound-guided parasternal intercostal nerve block for postoperative analgesia in patients undergoing median sternotomy for mediastinal mass resection.
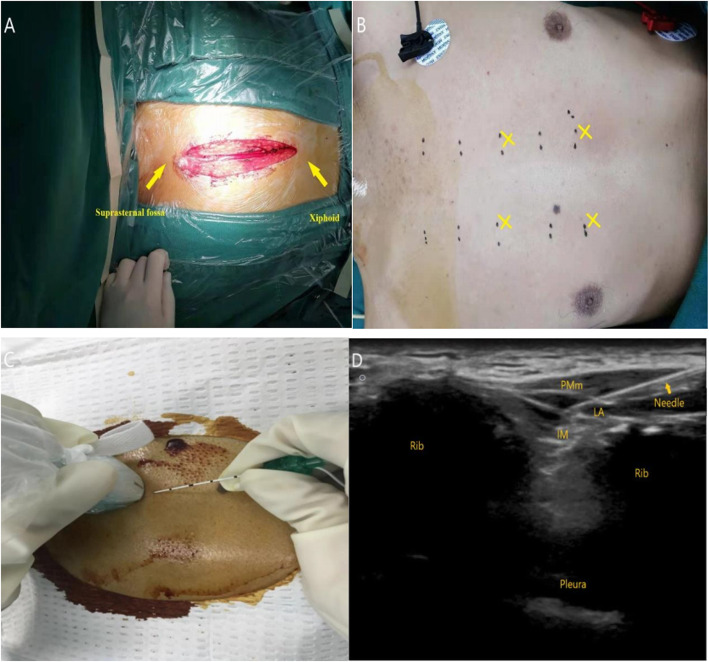
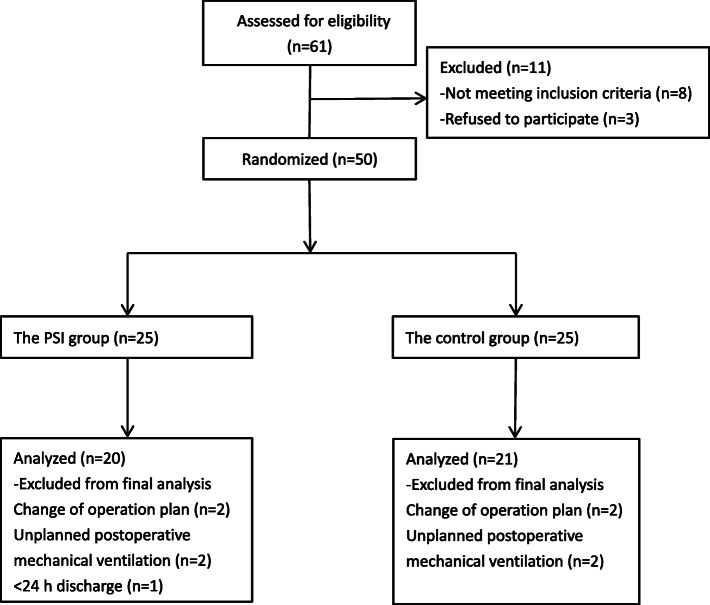
This randomized, double-blind, placebo-controlled trial performed in Renmin Hospital, Wuhan University, enrolled 41 participants aged 18-65 years. The patients scheduled for mediastinal mass resection by median sternotomy were randomly assigned were randomized into 2 groups, and preoperatively administered 2 injections of ropivacaine (PSI) and saline (control) groups, respectively, in the 3rd and 5th parasternal intercostal spaces with ultrasound-guided (USG) bilateral parasternal intercostal nerve block. Sufentanil via patient-controlled intravenous analgesia (PCIA) was administered to all participants postoperatively. Pain score, total sufentanil consumption, and postoperative adverse events were recorded within the first 24 h.
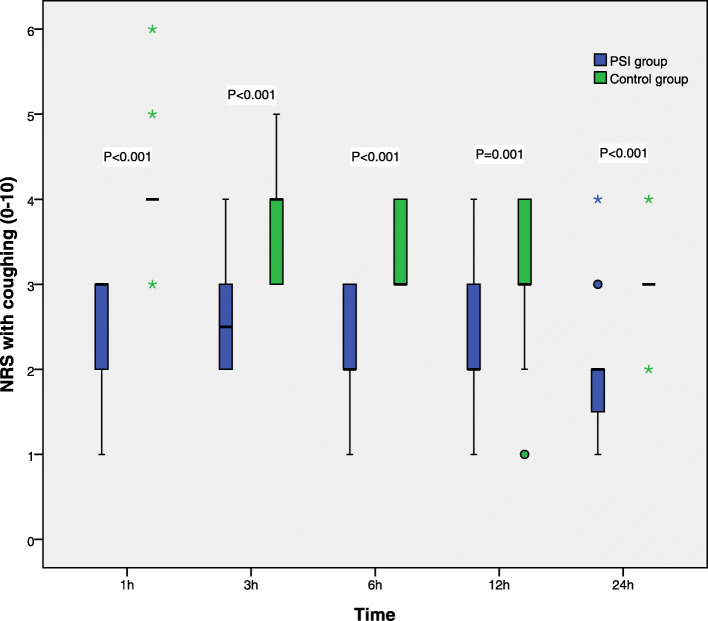
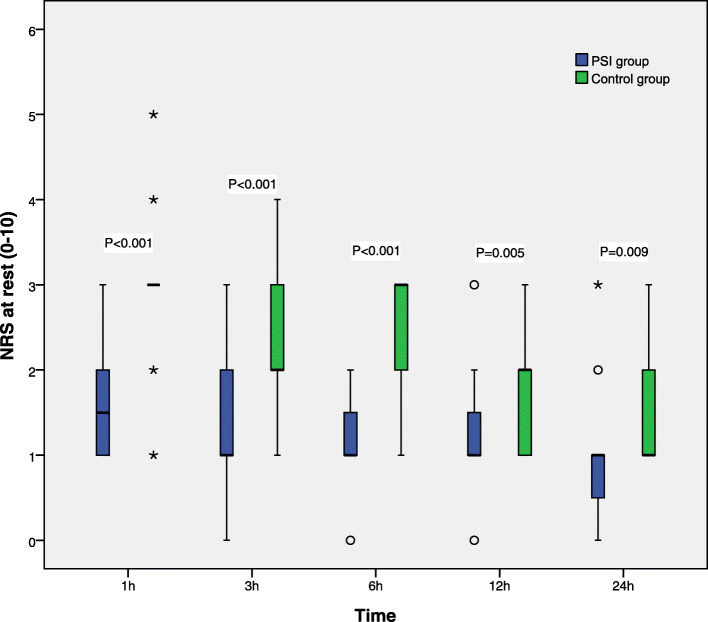
There were 20 and 21 patients in the PSI and control group, respectively. The PSI group required 20% less PCIA-sufentanil compared with the control group (54.05 ± 11.14 μg vs. 67.67 ± 8.92 μg, P < 0.001). In addition, pain numerical rating scale (NRS) scores were significantly lower in the PSI group compared with control patients, both at rest and upon coughing within 24 postoperative hours. Postoperative adverse events were generally reduced in the PSI group compared with controls.
USG bilateral parasternal intercostal nerve block effectively reduces postoperative pain and adjuvant analgesic requirement, with good patient satisfaction, therefore constituting a good option for mediastinal mass resection by median sternotomy.
经胸肋间隙神经阻滞在术后镇痛中很少使用,其价值尚不清楚。本研究旨在评估超声引导经胸肋间隙神经阻滞在胸骨正中切开术治疗纵隔肿块切除术后镇痛中的效果。
这项在武汉大学人民医院进行的随机、双盲、安慰剂对照试验纳入了 41 名年龄在 18-65 岁之间的患者。计划行胸骨正中切开术治疗纵隔肿块的患者被随机分为两组,分别在第 3 和第 5 肋间隙行超声引导(USG)双侧经胸肋间隙神经阻滞,术前分别给予罗哌卡因(PSI)和生理盐水(对照组)各 2 次注射。所有患者术后均给予舒芬太尼患者自控静脉镇痛(PCIA)。记录术后 24 小时内的疼痛评分、舒芬太尼总消耗量和术后不良反应。
PSI 组和对照组分别有 20 例和 21 例患者。PSI 组与对照组相比,PCIA-舒芬太尼的用量减少了 20%(54.05±11.14μg vs. 67.67±8.92μg,P<0.001)。此外,PSI 组患者在术后 24 小时内的静息和咳嗽时疼痛数字评分量表(NRS)评分均显著低于对照组。与对照组相比,PSI 组患者的术后不良反应总体减少。
USG 双侧经胸肋间隙神经阻滞可有效减轻术后疼痛和辅助镇痛需求,且患者满意度高,因此是胸骨正中切开术治疗纵隔肿块的一种较好选择。