Zotter Meredeth, Piechowiak Eike I, Balasubramaniam Rupashani, Von Martial Rascha, Genceviciute Kotryna, Blanquet Marisa, Slavova Nedelina, Sarikaya Hakan, Arnold Marcel, Gralla Jan, Jung Simon, Fischer Urs, El-Koussy Marwan, Heldner Mirjam R
Department of Neurology, Inselspital, University Hospital and University of Bern, Bern, Switzerland.
Institute of Diagnostic and Interventional Neuroradiology, Inselspital, University Hospital and University of Bern, Bern, Switzerland.
Ther Adv Neurol Disord. 2021 Mar 11;14:1756286421999017. doi: 10.1177/1756286421999017. eCollection 2021.
To investigate whether stroke aetiology affects outcome in patients with acute ischaemic stroke who undergo endovascular therapy.
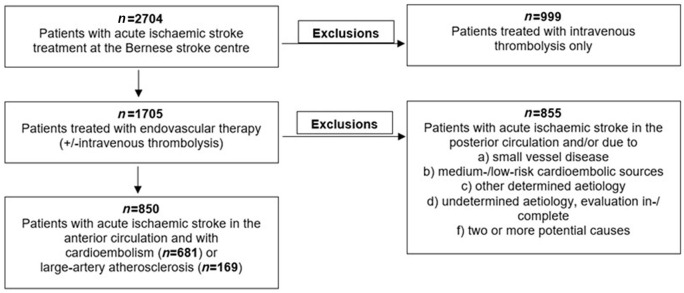
We retrospectively analysed patients from the Bernese Stroke Centre Registry (January 2010-September 2018), with acute large vessel occlusion in the anterior circulation due to cardioembolism or large-artery atherosclerosis, treated with endovascular therapy (±intravenous thrombolysis).
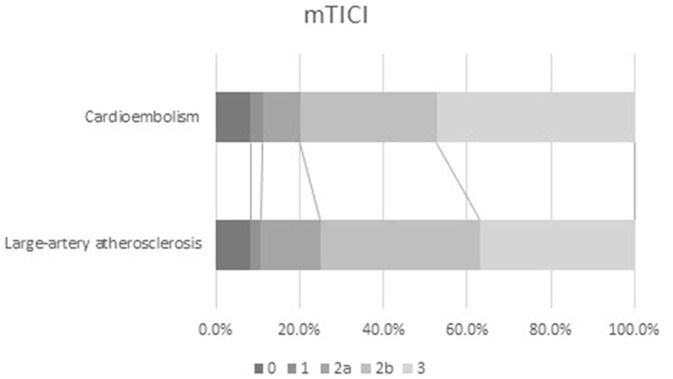
The study included 850 patients (median age 77.4 years, 49.3% female, 80.1% with cardioembolism). Compared with those with large-artery atherosclerosis, patients with cardioembolism were older, more often female, and more likely to have a history of hypercholesterolaemia, atrial fibrillation, current smoking (each < 0.0001) and higher median National Institutes of Health Stroke Scale (NIHSS) scores on admission ( = 0.030). They were more frequently treated with stent retrievers ( = 0.007), but the median number of stent retriever attempts was lower ( = 0.016) and fewer had permanent stent placements ( ⩽ 0.004). Univariable analysis showed that patients with cardioembolism had worse 3-month survival [72.7% 84%, odds ratio (OR) = 0.51; = 0.004] and modified Rankin scale (mRS) score shift ( = 0.043) and higher rates of post-interventional heart failure (33.5% 18.5%, OR = 2.22; < 0.0001), but better modified thrombolysis in cerebral infarction (mTICI) score shift ( = 0.025). Excellent (mRS = 0-1) 3-month outcome, successful reperfusion (mTICI = 2b-3), symptomatic intracranial haemorrhage and Updated Charlson Comorbidity Index were similar between groups. Propensity-matched analysis found no statistically significant difference in outcome between stroke aetiology groups. Stroke aetiology was not an independent predictor of favourable mRS score shift, but lower admission NIHSS score, younger age and independence pre-stroke were (each < 0.0001). Stroke aetiology was not an independent predictor of heart failure, but older age, admission antithrombotics and dependence pre-stroke were (each ⩽0.027). Stroke aetiology was not an independent predictor of favourable mTICI score shift, but application of stent retriever and no permanent intracranial stent placement were (each ⩽0.044).
We suggest prospective studies to further elucidate differences in reperfusion and outcome between patients with cardioembolism and large-artery atherosclerosis.
探讨卒中病因是否会影响接受血管内治疗的急性缺血性卒中患者的预后。
我们回顾性分析了伯尔尼卒中中心登记处(2010年1月至2018年9月)因心源性栓塞或大动脉粥样硬化导致前循环急性大血管闭塞并接受血管内治疗(±静脉溶栓)的患者。
该研究纳入了850例患者(中位年龄77.4岁,49.3%为女性,80.1%有心源性栓塞)。与大动脉粥样硬化患者相比,心源性栓塞患者年龄更大,女性更常见,更可能有高胆固醇血症、心房颤动、当前吸烟史(均<0.0001),入院时美国国立卫生研究院卒中量表(NIHSS)中位评分更高(=0.030)。他们更常接受取栓支架治疗(=0.007),但取栓支架尝试的中位次数更低(=0.016),永久性支架置入的患者更少(⩽0.004)。单因素分析显示,心源性栓塞患者3个月生存率更低[72.7%对84%,比值比(OR)=0.51;=0.004],改良Rankin量表(mRS)评分变化更差(=0.043),介入后心力衰竭发生率更高(33.5%对18.5%,OR=2.22;<0.0001),但改良脑梗死溶栓(mTICI)评分变化更好(=0.025)。两组间3个月良好预后(mRS=0 - 1)、成功再灌注(mTICI=2b - 3)、症状性颅内出血和更新的Charlson合并症指数相似。倾向匹配分析发现卒中病因组之间的预后无统计学显著差异。卒中病因不是mRS评分良好变化的独立预测因素,但入院时NIHSS评分更低、年龄更小和卒中前独立状态是(均<0.0001)。卒中病因不是心力衰竭的独立预测因素,但年龄更大、入院时使用抗栓药物和卒中前依赖状态是(均⩽0.027)。卒中病因不是mTICI评分良好变化的独立预测因素,但使用取栓支架和无永久性颅内支架置入是(均⩽0.044)。
我们建议进行前瞻性研究,以进一步阐明心源性栓塞和大动脉粥样硬化患者在再灌注和预后方面的差异。