Fan Xiaona, Wang Dan, Zhang Wenjing, Liu Jinshuang, Liu Chao, Li Qingwei, Ma Zhigang, Li Hengzhen, Guan Xin, Bai Yibing, Yang Jiani, Lou Changjie, Li Xiaobo, Wang Guangyu, Li Zhiwei
Department of Gastrointestinal Medical Oncology, Harbin Medical University Cancer Hospital, Harbin, China.
Translational Medicine Research and Cooperation Center of Northern China, Heilongjiang Academy of Medical Sciences, Harbin, China.
Front Cell Dev Biol. 2021 Mar 15;9:638312. doi: 10.3389/fcell.2021.638312. eCollection 2021.
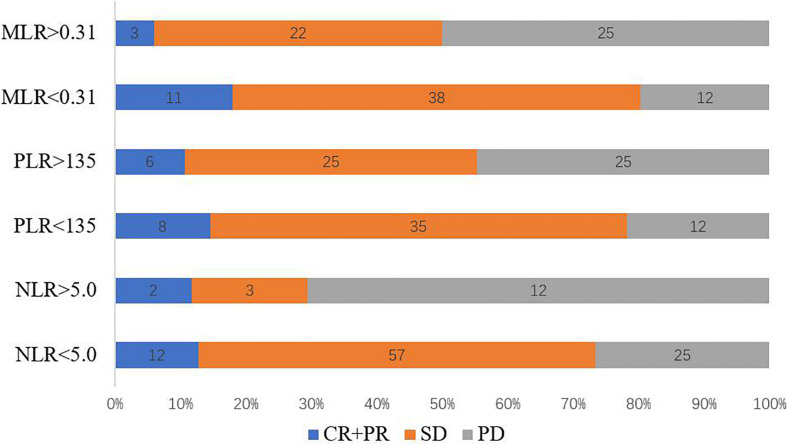
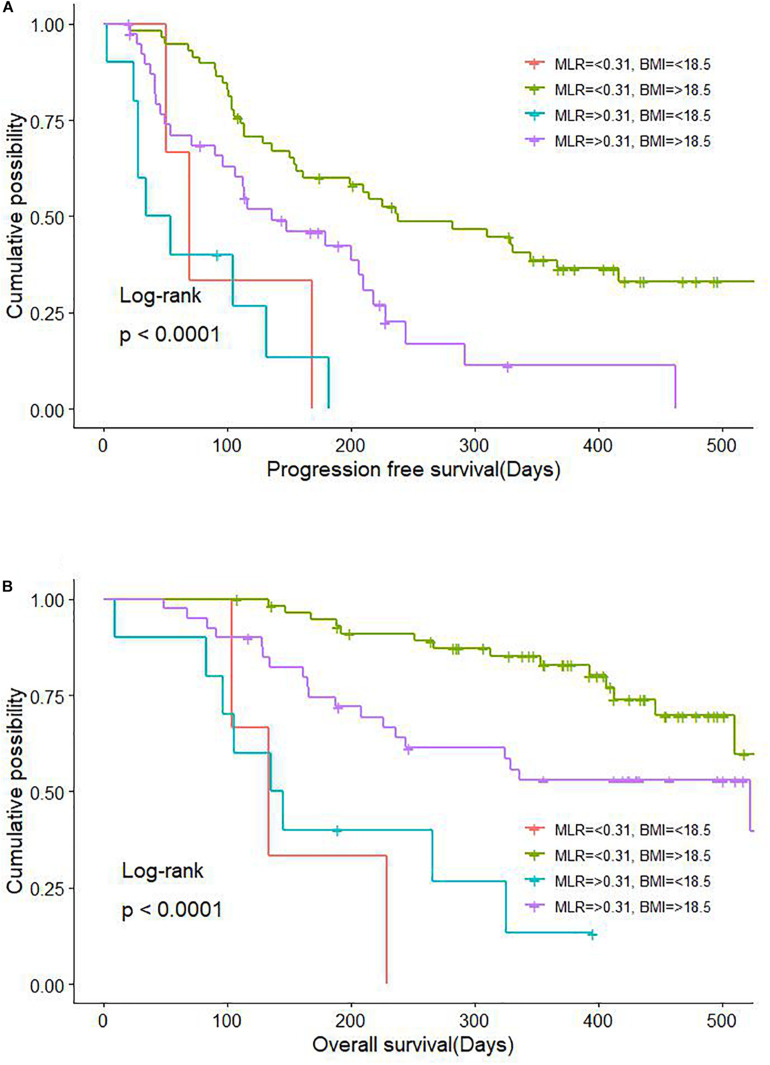
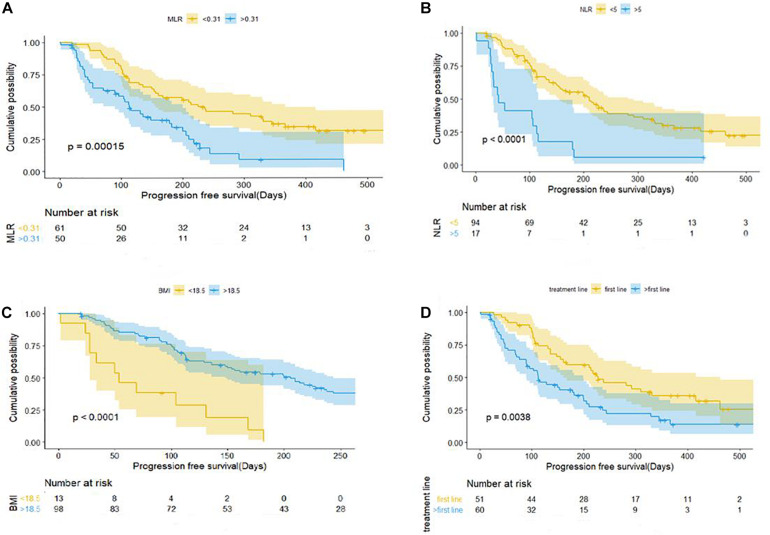
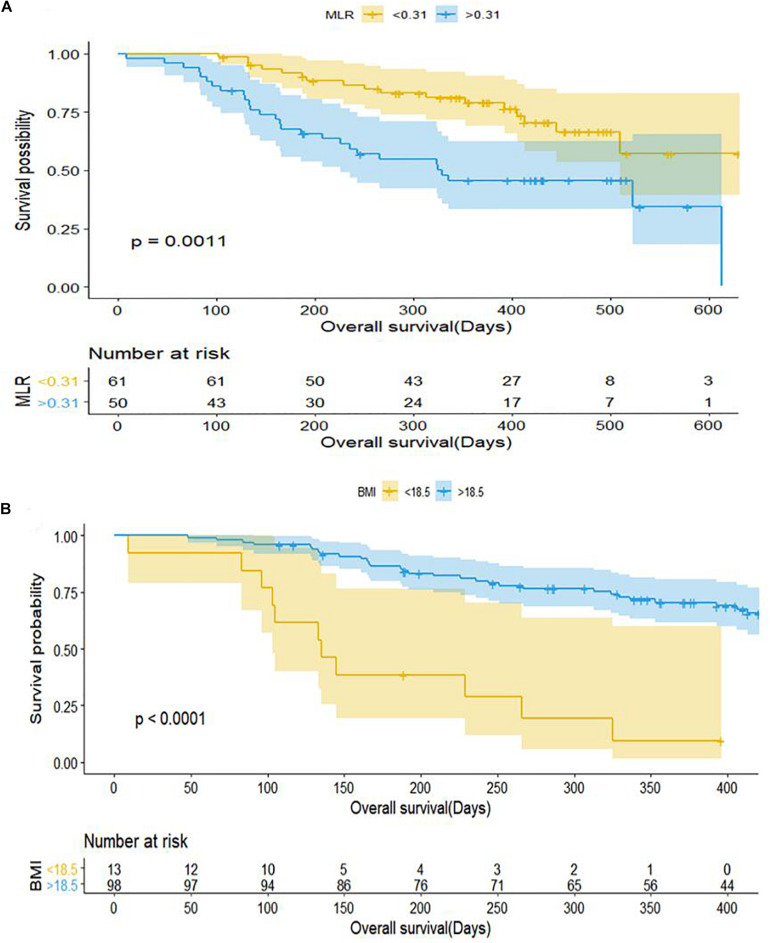
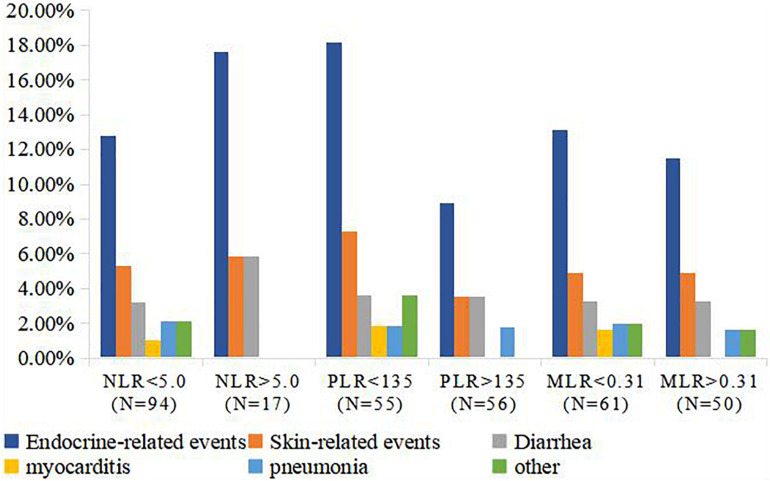
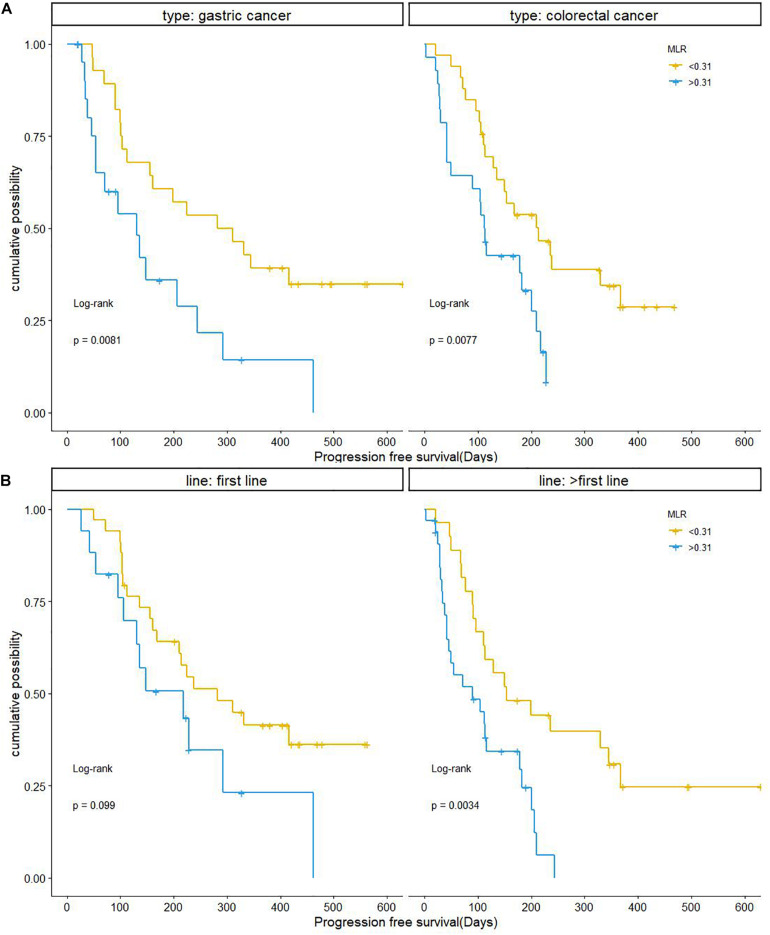
There is a lack of useful biomarkers for predicting the efficacy of anti-programmed death-1 (PD-1) therapy for advanced gastric and colorectal cancer. To address this issue, in this study we investigated the correlation between inflammatory marker expression and survival in patients with advanced gastric and colorectal cancer. Data for 111 patients with advanced gastric and colorectal cancer treated with anti-PD-1 regimens were retrospectively analyzed. Neutrophil-to-lymphocyte ratio (NLR), monocyte-to-lymphocyte ratio (MLR), platelet-to-lymphocyte ratio (PLR), and clinical characteristics of each patient were selected as the main variables. Overall response rate, disease control rate, and progression-free survival were primary endpoints, and overall survival and immune-related adverse events (irAEs) were secondary endpoints. The chi-squared test and Fisher's exact test were used to evaluate relationships between categorical variables. Uni- and multivariate Cox regression analyses were performed, and median progression-free survival and overall survival were estimated with the Kaplan-Meier method. The overall response rate and disease control rate of anti-PD-1therapy in advanced gastric and colorectal tumors were 12.61 and 66.66%, respectively. The patients with MLR < 0.31, NLR < 5, and PLR < 135 had a significantly higher disease control rate than those with MLR > 0.31, NLR > 5, and PLR > 135 ( < 0.05). The multivariate analysis revealed that MLR < 0.31, BMI > 18.5, and anti-PD-1 therapy in first-line were associated with prolonged PFS. MLR < 0.31 and BMI > 18.5 were associated with prolonged overall survival. The irAE rate differed significantly between PLR groups, and PLR < 135 was associated with an increased rate of irAEs ( = 0.028). These results indicate that the inflammatory markers NLR, MLR, and PLR have clinical utility for predicting survival or risk of irAEs in patients with advanced gastric cancer and colorectal cancer.
目前缺乏可用于预测晚期胃癌和结直肠癌抗程序性死亡-1(PD-1)治疗疗效的有效生物标志物。为解决这一问题,在本研究中,我们调查了晚期胃癌和结直肠癌患者炎症标志物表达与生存之间的相关性。对111例接受抗PD-1方案治疗的晚期胃癌和结直肠癌患者的数据进行了回顾性分析。选择中性粒细胞与淋巴细胞比值(NLR)、单核细胞与淋巴细胞比值(MLR)、血小板与淋巴细胞比值(PLR)以及每位患者的临床特征作为主要变量。总缓解率、疾病控制率和无进展生存期为主要终点,总生存期和免疫相关不良事件(irAE)为次要终点。采用卡方检验和Fisher精确检验评估分类变量之间的关系。进行单因素和多因素Cox回归分析,并用Kaplan-Meier法估计中位无进展生存期和总生存期。晚期胃癌和结直肠癌抗PD-1治疗的总缓解率和疾病控制率分别为12.61%和66.66%。MLR<0.31、NLR<5和PLR<135的患者疾病控制率显著高于MLR>0.31、NLR>5和PLR>135的患者(P<0.05)。多因素分析显示,MLR<0.31、BMI>18.5以及一线接受抗PD-1治疗与PFS延长相关。MLR<0.31和BMI>18.5与总生存期延长相关。PLR组之间的irAE发生率差异显著,PLR<135与irAE发生率增加相关(P=0.028)。这些结果表明,炎症标志物NLR、MLR和PLR在预测晚期胃癌和结直肠癌患者的生存或irAE风险方面具有临床应用价值。