Department of Neurosciences, Barrow Neurological Institute At Phoenix Children's Hospital, 1919 E. Thomas Road, Ambulatory Building B, 3rd floor, Phoenix, AZ, 85016, USA.
Department of Child Health, University Arizona College of Medicine -Phoenix, 550 E. Van Buren Street, Phoenix, AZ, 85004, USA.
Neurocrit Care. 2021 Aug;35(1):3-15. doi: 10.1007/s12028-021-01190-8. Epub 2021 Mar 31.
BACKGROUND/OBJECTIVE: Multimodality neurologic monitoring (MMM) is an emerging technique for management of traumatic brain injury (TBI). An increasing array of MMM-derived biomarkers now exist that are associated with injury severity and functional outcomes after TBI. A standardized MMM reporting process has not been well described, and a paucity of evidence exists relating MMM reporting in TBI management with functional outcomes or adverse events.
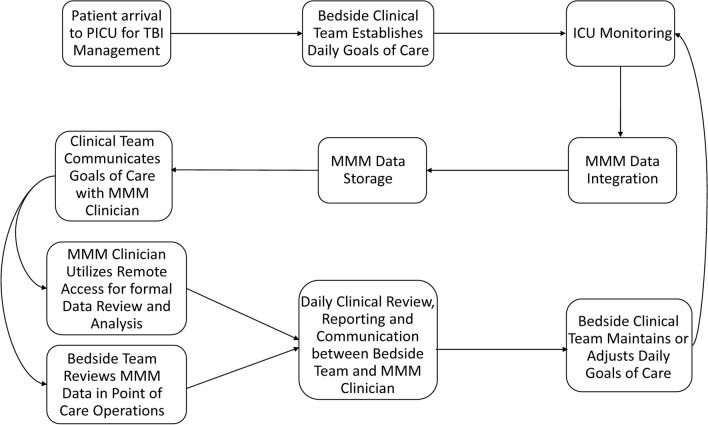
Prospective implementation of standardized MMM reporting at a single pediatric intensive care unit (PICU) is described that included monitoring of intracranial pressure (ICP), cerebral oxygenation and electroencephalography (EEG). The incidence of clinical decisions made using MMM reporting is described, including timing of neuroimaging, ICP monitoring discontinuation, use of paralytic, hyperosmolar and pentobarbital therapies, neurosurgical interventions, ventilator and CPP adjustments and neurologic prognostication discussions. Retrospective analysis was performed on the association of MMM reporting with initial Glasgow Coma Scale (GCS) and Pediatric Risk of Mortality III (PRISM III) scores, duration of total hospitalization and PICU hospitalization, duration of mechanical ventilation and invasive ICP monitoring, inpatient complications, time with ICP > 20 mmHg, time with cerebral perfusion pressure (CPP) < 40 mmHg and 12-month Glasgow Outcome Scale-Extended Pediatrics (GOSE-Peds) scores. Association of outcomes with MMM reporting was investigated using the Wilcoxon rank-sum test or Fisher's exact test, as appropriate.
Eighty-five children with TBI underwent MMM over 6 years, among which 18 underwent daily MMM reporting over a 21-month period. Clinical decision-making influenced by MMM reporting included timing of neuroimaging (100.0%), ICP monitoring discontinuation (100.0%), timing of extubation trials of surviving patients (100.0%), body repositioning (11.1%), paralytic therapy (16.7%), hyperosmolar therapy (22.2%), pentobarbital therapy (33.3%), provocative cerebral autoregulation testing (16.7%), adjustments in CPP thresholds (16.7%), adjustments in PaCO2 thresholds (11.1%), neurosurgical interventions (16.7%) and neurologic prognostication discussions (11.1%). The implementation of MMM reporting was associated with a reduction in ICP monitoring duration (p = 0.0017) and mechanical ventilator duration (p = 0.0018). No significant differences were observed in initial GCS or PRISM III scores, total hospitalization length, PICU hospitalization length, total complications, time with ICP > 20 mmHg, time with CPP < 40 mmHg, use of tier 2 therapy, or 12-month GOS-E Peds scores.
Implementation of MMM reporting in pediatric TBI management is feasible and can be impactful in tailoring clinical decisions. Prospective work is needed to understand the impact of MMM and MMM reporting systems on functional outcomes and clinical care efficacy.
背景/目的:多模态神经监测(MMM)是一种新兴的创伤性脑损伤(TBI)管理技术。现在已经存在越来越多的与 TBI 后损伤严重程度和功能结果相关的 MMM 衍生生物标志物。尚未很好地描述标准化的 MMM 报告流程,并且关于 TBI 管理中 MMM 报告与功能结果或不良事件之间的关系,证据也很少。
描述了在单一儿科重症监护病房(PICU)中实施标准化 MMM 报告的前瞻性方法,其中包括颅内压(ICP)、脑氧合和脑电图(EEG)监测。描述了使用 MMM 报告做出的临床决策的发生率,包括神经影像学检查的时机、ICP 监测的停止、使用麻痹剂、高渗剂和戊巴比妥治疗、神经外科干预、呼吸机和 CPP 调整以及神经预后讨论。对 MMM 报告与初始格拉斯哥昏迷量表(GCS)和儿科死亡率 III 评分(PRISM III)、总住院时间和 PICU 住院时间、机械通气和有创 ICP 监测时间、住院并发症、ICP>20mmHg 时间、CPP<40mmHg 时间和 12 个月格拉斯哥结局量表-扩展儿科(GOSE-Peds)评分的相关性进行了回顾性分析。使用 Wilcoxon 秩和检验或 Fisher 确切检验(视情况而定)对结果与 MMM 报告的相关性进行了研究。
85 名 TBI 患儿在 6 年内接受了 MMM,其中 18 名患儿在 21 个月期间接受了每日 MMM 报告。受 MMM 报告影响的临床决策包括神经影像学检查的时机(100.0%)、ICP 监测的停止(100.0%)、存活患者拔管试验的时机(100.0%)、体位调整(11.1%)、麻痹剂治疗(16.7%)、高渗剂治疗(22.2%)、戊巴比妥治疗(33.3%)、刺激性脑自动调节测试(16.7%)、CPP 阈值调整(16.7%)、PaCO2 阈值调整(11.1%)、神经外科干预(16.7%)和神经预后讨论(11.1%)。实施 MMM 报告与减少 ICP 监测时间(p=0.0017)和机械通气时间(p=0.0018)相关。初始 GCS 或 PRISM III 评分、总住院时间、PICU 住院时间、总并发症、ICP>20mmHg 时间、CPP<40mmHg 时间、使用 2 级治疗或 12 个月 GOS-E Peds 评分无显著差异。
在儿科 TBI 管理中实施 MMM 报告是可行的,并可以对临床决策产生影响。需要前瞻性工作来了解 MMM 及其报告系统对功能结果和临床护理效果的影响。