World Health Organization, Geneva, Switzerland.
Institute of Global Health, Faculty of Medicine, University of Geneva, Geneva, Switzerland.
PLoS Med. 2021 Apr 1;18(4):e1003587. doi: 10.1371/journal.pmed.1003587. eCollection 2021 Apr.
Unrest in Myanmar in August 2017 resulted in the movement of over 700,000 Rohingya refugees to overcrowded camps in Cox's Bazar, Bangladesh. A large outbreak of diphtheria subsequently began in this population.
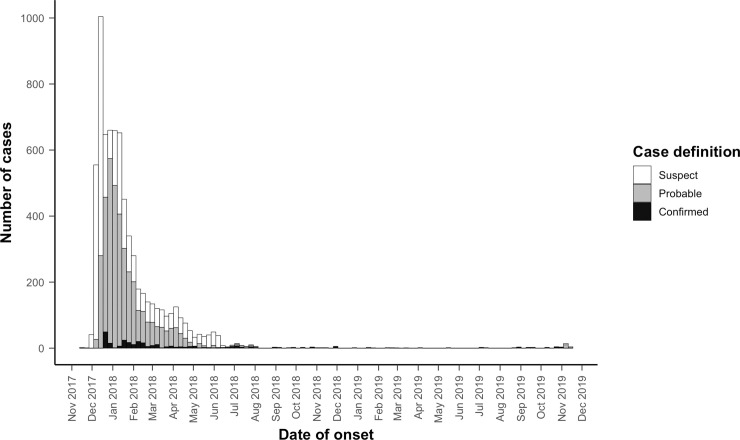
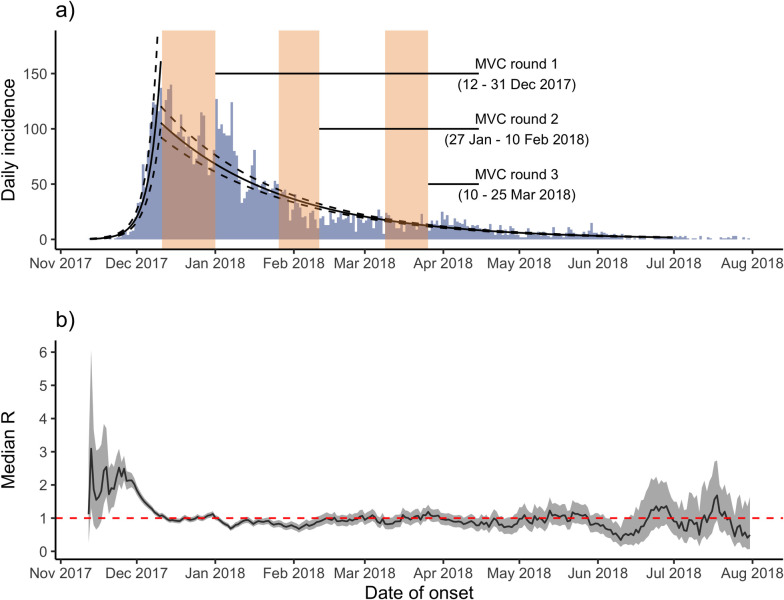
Data were collected during mass vaccination campaigns (MVCs), contact tracing activities, and from 9 Diphtheria Treatment Centers (DTCs) operated by national and international organizations. These data were used to describe the epidemiological and clinical features and the control measures to prevent transmission, during the first 2 years of the outbreak. Between November 10, 2017 and November 9, 2019, 7,064 cases were reported: 285 (4.0%) laboratory-confirmed, 3,610 (51.1%) probable, and 3,169 (44.9%) suspected cases. The crude attack rate was 51.5 cases per 10,000 person-years, and epidemic doubling time was 4.4 days (95% confidence interval [CI] 4.2-4.7) during the exponential growth phase. The median age was 10 years (range 0-85), and 3,126 (44.3%) were male. The typical symptoms were sore throat (93.5%), fever (86.0%), pseudomembrane (34.7%), and gross cervical lymphadenopathy (GCL; 30.6%). Diphtheria antitoxin (DAT) was administered to 1,062 (89.0%) out of 1,193 eligible patients, with adverse reactions following among 229 (21.6%). There were 45 deaths (case fatality ratio [CFR] 0.6%). Household contacts for 5,702 (80.7%) of 7,064 cases were successfully traced. A total of 41,452 contacts were identified, of whom 40,364 (97.4%) consented to begin chemoprophylaxis; adherence was 55.0% (N = 22,218) at 3-day follow-up. Unvaccinated household contacts were vaccinated with 3 doses (with 4-week interval), while a booster dose was administered if the primary vaccination schedule had been completed. The proportion of contacts vaccinated was 64.7% overall. Three MVC rounds were conducted, with administrative coverage varying between 88.5% and 110.4%. Pentavalent vaccine was administered to those aged 6 weeks to 6 years, while tetanus and diphtheria (Td) vaccine was administered to those aged 7 years and older. Lack of adequate diagnostic capacity to confirm cases was the main limitation, with a majority of cases unconfirmed and the proportion of true diphtheria cases unknown.
To our knowledge, this is the largest reported diphtheria outbreak in refugee settings. We observed that high population density, poor living conditions, and fast growth rate were associated with explosive expansion of the outbreak during the initial exponential growth phase. Three rounds of mass vaccinations targeting those aged 6 weeks to 14 years were associated with only modestly reduced transmission, and additional public health measures were necessary to end the outbreak. This outbreak has a long-lasting tail, with Rt oscillating at around 1 for an extended period. An adequate global DAT stockpile needs to be maintained. All populations must have access to health services and routine vaccination, and this access must be maintained during humanitarian crises.
2017 年 8 月,缅甸发生动乱,超过 70 万罗兴亚难民涌入孟加拉国 Cox's Bazar 拥挤的难民营。随后,该地区爆发了大规模白喉疫情。
数据收集自大规模疫苗接种活动(MVC)、接触者追踪活动,以及由国家和国际组织运营的 9 个白喉治疗中心(DTC)。这些数据用于描述疫情爆发的前 2 年的流行病学和临床特征,以及预防传播的控制措施。2017 年 11 月 10 日至 2019 年 11 月 9 日,共报告了 7064 例病例:285 例(4.0%)实验室确诊,3610 例(51.1%)可能病例,3169 例(44.9%)疑似病例。粗发病率为每 10000 人年 51.5 例,指数增长阶段的暴发倍增时间为 4.4 天(95%置信区间[CI]为 4.2-4.7)。中位数年龄为 10 岁(范围 0-85),3126 例(44.3%)为男性。典型症状为咽痛(93.5%)、发热(86.0%)、假膜(34.7%)和明显颈部淋巴结病(GCL;30.6%)。1193 名符合条件的患者中有 1062 名(89.0%)接受了白喉抗毒素(DAT)治疗,其中 229 名(21.6%)出现不良反应。共有 45 人死亡(病死率[CFR]为 0.6%)。5702 例(80.7%)病例的家庭接触者被成功追踪。共发现 41452 名接触者,其中 40364 名(97.4%)同意开始化学预防;3 天随访时,依从性为 55.0%(N=22218)。未接种疫苗的家庭接触者接种了 3 剂(间隔 4 周),如果已完成基础免疫接种计划,则给予加强剂量。总体接触者接种比例为 64.7%。共进行了 3 轮大规模疫苗接种活动,行政覆盖率在 88.5%至 110.4%之间。6 周至 6 岁的儿童接种五联疫苗,7 岁及以上的儿童接种破伤风和白喉(Td)疫苗。确认病例的能力不足是主要限制因素,大多数病例未经确认,真实白喉病例的比例未知。
据我们所知,这是有记录以来在难民环境中发生的最大规模的白喉疫情。我们观察到,人口密度高、生活条件差和快速增长率与疫情在初始指数增长阶段的迅速扩大有关。针对 6 周至 14 岁儿童的三轮大规模疫苗接种活动仅略微降低了传播速度,还需要采取其他公共卫生措施来结束疫情。此次疫情有一个较长的尾巴,Rt 在很长一段时间内都在 1 左右波动。需要维持足够的全球 DAT 储备。所有人群都必须获得卫生服务和常规疫苗接种,并且必须在人道主义危机期间维持这种获得途径。