Emory University School of Medicine, Atlanta, Georgia.
ECOG-ACRIN Biostatistics Center, Dana-Farber Cancer Institute, Boston, Massachusetts.
Cancer. 2021 Jul 15;127(14):2545-2552. doi: 10.1002/cncr.33527. Epub 2021 Apr 1.
Early discontinuation is a substantial barrier to the delivery of endocrine therapies (ETs) and may influence recurrence and survival. The authors investigated the association between early discontinuation of ET and social determinants of health, including insurance coverage and the neighborhood deprivation index (NDI), which was measured on the basis of patients' zip codes, in breast cancer.
In this retrospective analysis of a prospective randomized clinical trial (Trial Assigning Individualized Options for Treatment), women with hormone receptor-positive, human epidermal growth factor receptor 2-negative breast cancer who started ET within a year of study entry were included. Early discontinuation was calculated as stopping ET within 4 years of its start for reasons other than distant recurrence or death via Kaplan-Meier estimates. A Cox proportional hazards joint model was used to analyze the association between early discontinuation of ET and factors such as the study-entry insurance and NDI, with adjustments made for other variables.
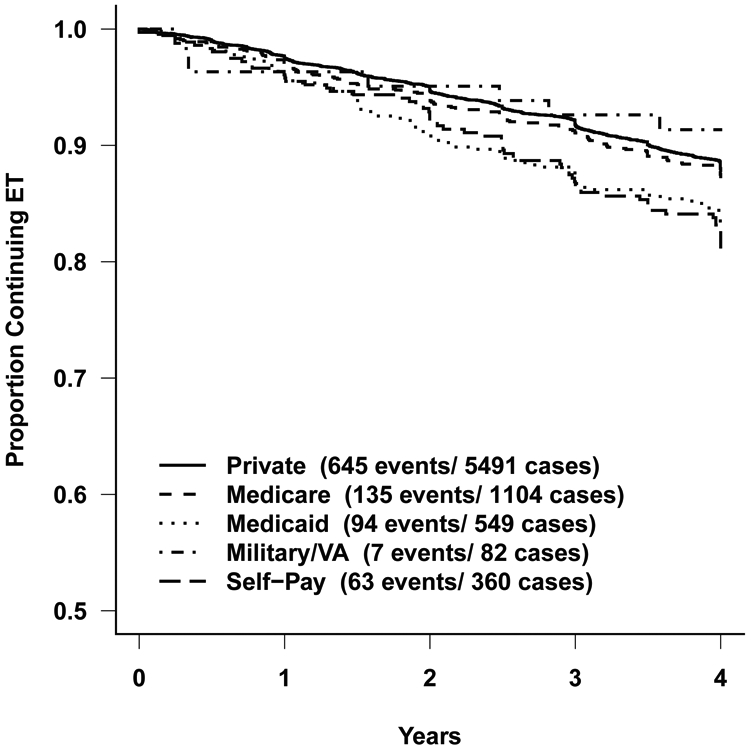
Of the included 9475 women (mean age, 55.6 years; White race, 84%), 58.0% had private insurance, whereas 11.7% had Medicare, 5.8% had Medicaid, 3.8% were self-pay, and 19.1% were treated at international sites. The early discontinuation rate was 12.3%. Compared with those with private insurance, patients with Medicaid (hazard ratio [HR], 1.53; 95% confidence interval [CI], 1.23-1.92) and self-pay patients (HR, 1.65; 95% CI, 1.25-2.17) had higher early discontinuation. Participants with a first-quartile NDI (highest deprivation) had a higher probability of discontinuation than those with a fourth-quartile NDI (lowest deprivation; HR, 1.34; 95% CI, 1.11-1.62).
Patients' insurance and zip code at study entry play roles in adherence to ET, with uninsured and underinsured patients having a high rate of treatment nonadherence. Early identification of patients at risk may improve adherence to therapy.
In this retrospective analysis of 9475 women with breast cancer participating in a clinical trial (Trial Assigning Individualized Options for Treatment), Medicaid and self-pay patients (compared with those with private insurance) and those in the highest quartile of neighborhood deprivation scores (compared with those in the lowest quartile) had a higher probability of early discontinuation of endocrine therapy. These social determinants of health assume larger importance with the expected increase in unemployment rates and loss of insurance coverage in the aftermath of the coronavirus disease 2019 pandemic. Early identification of patients at risk and enrollment in insurance optimization programs may improve the persistence of therapy.
早期停药是内分泌治疗(ET)实施的一个重大障碍,可能会影响复发和生存。作者研究了早期停药与健康的社会决定因素(包括保险覆盖范围和邻里剥夺指数[NDI])之间的关系,NDI 是基于患者的邮政编码来衡量的,该研究纳入了乳腺癌患者。
本回顾性分析纳入了一项前瞻性随机临床试验(Trial Assigning Individualized Options for Treatment)中,在研究入组后一年内开始 ET 的激素受体阳性、人表皮生长因子受体 2 阴性乳腺癌患者。通过 Kaplan-Meier 估计,早期停药定义为 ET 开始后 4 年内因远处复发或死亡以外的原因停药。采用 Cox 比例风险联合模型分析 ET 早期停药与研究入组时的保险和 NDI 等因素之间的关系,并对其他变量进行调整。
在纳入的 9475 名女性(平均年龄 55.6 岁;白人 84%)中,58.0%有私人保险,11.7%有医疗保险,5.8%有医疗补助,3.8%是自费,19.1%在国际站点接受治疗。早期停药率为 12.3%。与有私人保险的患者相比,有医疗补助(风险比[HR],1.53;95%置信区间[CI],1.23-1.92)和自费患者(HR,1.65;95%CI,1.25-2.17)的早期停药率更高。NDI 第一四分位数(最高剥夺)的参与者停药的可能性高于 NDI 第四四分位数(最低剥夺)的参与者(HR,1.34;95%CI,1.11-1.62)。
患者在研究入组时的保险和邮政编码对 ET 的依从性有影响,无保险和保险不足的患者治疗依从性较差。早期识别有风险的患者可能会提高治疗的依从性。
NDI(Neighborhood Deprivation Index)为邻里剥夺指数。