Sashindranath Maithili, Nandurkar Harshal H
Australian Centre for Blood Diseases, Central Clinical School, Monash University and Alfred Health, Melbourne, VIC, Australia.
Stroke. 2021 May;52(5):1895-1904. doi: 10.1161/STROKEAHA.120.032711. Epub 2021 Apr 2.
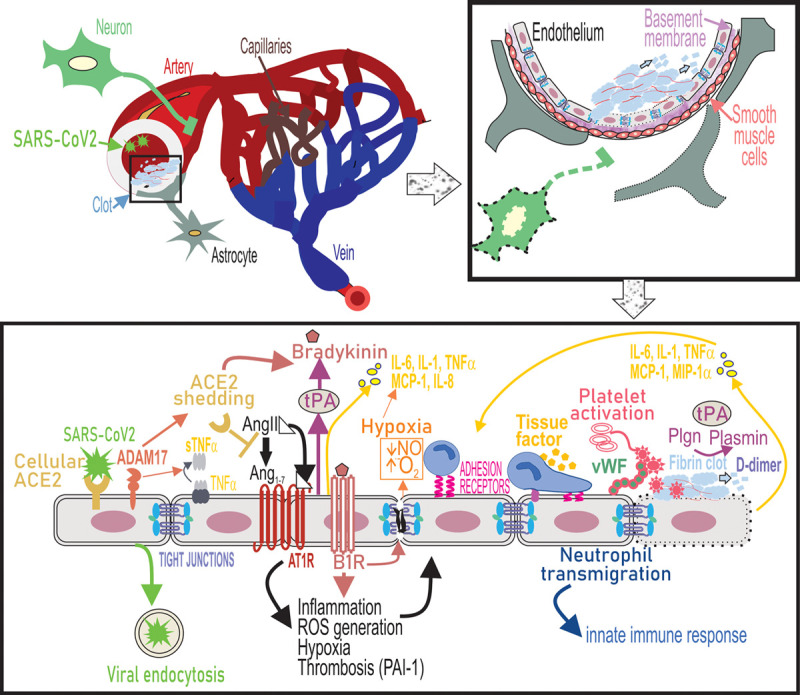
The Coronavirus disease 2019 (COVID)-19 pandemic has already affected millions worldwide, with a current mortality rate of 2.2%. While it is well-established that severe acute respiratory syndrome-coronavirus-2 causes upper and lower respiratory tract infections, a number of neurological sequelae have now been reported in a large proportion of cases. Additionally, the disease causes arterial and venous thromboses including pulmonary embolism, myocardial infarction, and a significant number of cerebrovascular complications. The increasing incidence of large vessel ischemic strokes as well as intracranial hemorrhages, frequently in younger individuals, and associated with increased morbidity and mortality, has raised questions as to why the brain is a major target of the disease. COVID-19 is characterized by hypercoagulability with alterations in hemostatic markers including high D-dimer levels, which are a prognosticator of poor outcome. Together with findings of fibrin-rich microthrombi, widespread extracellular fibrin deposition in affected various organs and hypercytokinemia, this suggests that COVID-19 is more than a pulmonary viral infection. Evidently, COVID-19 is a thrombo-inflammatory disease. Endothelial cells that constitute the lining of blood vessels are the primary targets of a thrombo-inflammatory response, and severe acute respiratory syndrome coronavirus 2 also directly infects endothelial cells through the ACE2 (angiotensin-converting enzyme 2) receptor. Being highly heterogeneous in their structure and function, differences in the endothelial cells may govern the susceptibility of organs to COVID-19. Here, we have explored how the unique characteristics of the cerebral endothelium may be the underlying reason for the increased rates of cerebrovascular pathology associated with COVID-19.
2019年冠状病毒病(COVID-19)大流行已经影响了全球数百万人,目前的死亡率为2.2%。虽然严重急性呼吸综合征冠状病毒2会引发上、下呼吸道感染这一点已得到充分证实,但现在已有大量病例报告出现了一些神经后遗症。此外,该疾病还会导致动脉和静脉血栓形成,包括肺栓塞、心肌梗死以及大量脑血管并发症。大血管缺血性中风以及颅内出血的发病率不断上升,且经常发生在较年轻的个体中,并伴有发病率和死亡率的增加,这引发了关于为何大脑是该疾病主要靶器官的疑问。COVID-19的特征是具有高凝性,凝血标志物发生改变,包括D-二聚体水平升高,这是预后不良的一个预测指标。连同富含纤维蛋白的微血栓形成、受影响的各个器官中广泛的细胞外纤维蛋白沉积以及高细胞因子血症的发现,这表明COVID-19不仅仅是一种肺部病毒感染。显然,COVID-19是一种血栓炎症性疾病。构成血管内衬的内皮细胞是血栓炎症反应的主要靶标,严重急性呼吸综合征冠状病毒2还通过血管紧张素转换酶2(ACE2)受体直接感染内皮细胞。内皮细胞在结构和功能上高度异质性,其差异可能决定器官对COVID-19的易感性。在此,我们探讨了脑内皮细胞的独特特征如何可能是与COVID-19相关的脑血管病变发生率增加的根本原因。