Li Hao, Ye Shi-Sheng, Wu Yuan-Ling, Huang Sheng-Ming, Li Yong-Xin, Lu Kui, Huang Jing-Bo, Chen Lve, Li Hong-Zhuang, Wu Wen-Jun, Wu Zhi-Lin, Wu Jian-Zhou, Zhong Wang-Tao, Xian Wen-Chuan, Liao Feng, Tung Tao-Hsin, Wu Qiao-Ling, Chen Hai, Yuan Li, Yang Zhi, Huang Li-An
Department of Neurology, Maoming People's Hospital, Maoming, China.
Department of Neurology, Longgang District People's Hospital of Shenzhen, Shenzhen, China.
BMJ Open. 2021 Apr 1;11(4):e043415. doi: 10.1136/bmjopen-2020-043415.
We aimed to determine predictors of mortality within 90 days and develop a simple score for patients with mechanical thrombectomy (MT).
Analysis of a multicentre prospective registry.
In six participating centres, patients who had an acute ischaemic stroke (AIS) treated by MT between March 2017 and May 2018 were documented prospectively.
224 patients with AIS were treated by MT.
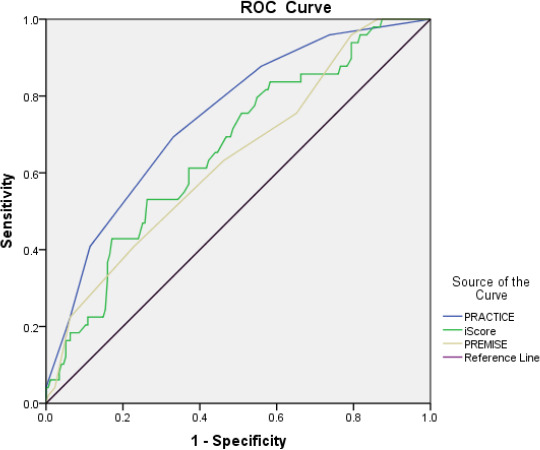
Of 224 patients, 49 (21.9%) patients died, and 87 (38.8%) were independent. Variables associated with 90-day mortality were age, previous stroke, admission National Institutes of Health Stroke Scale (NIHSS), fasting blood glucose and occlusion site. Logistic regression identified four variables independently associated with 90-day mortality: age ≥80 years (OR 3.26, 95% CI 1.45 to 7.33), previous stroke (OR 2.33, 95% CI 1.04 to 5.21), admission NIHSS ≥18 (OR 2.37, 95% CI 1.13 to 4.99) and internal carotid artery or basilar artery occlusion (OR 2.92, 95% CI 1.34 to 6.40). Using these data, we developed predicting 90-day mortality of AIS with MT (PRACTICE) score ranging from 0 to 6 points. The receiver operator curve analysis found that PRACTICE score (area under the curve (AUC)=0.744, 95% CI 0.669 to 0.820) was numerically better than iScore (AUC=0.661, 95% CI 0.577 to 0.745) and Predicting Early Mortality of Ischemic Stroke score (AUC=0.638, 95% CI 0.551 to 0.725) for predicting 90-day mortality.
We developed a simple score to estimate the 90-day mortality of patients who had an AIS treated with MT. But the score needs to be prospectively validated.
Chinese Clinical Trial Registry (ChiCTR-OOC-17013052).
我们旨在确定90天内的死亡预测因素,并为接受机械取栓术(MT)的患者制定一个简单的评分系统。
对多中心前瞻性登记数据进行分析。
在六个参与中心,对2017年3月至2018年5月期间接受MT治疗的急性缺血性卒中(AIS)患者进行前瞻性记录。
224例AIS患者接受了MT治疗。
224例患者中,49例(21.9%)死亡,87例(38.8%)功能独立。与90天死亡率相关的变量有年龄、既往卒中史、入院时美国国立卫生研究院卒中量表(NIHSS)评分、空腹血糖和闭塞部位。逻辑回归分析确定了与90天死亡率独立相关的四个变量:年龄≥80岁(比值比[OR]3.26,95%置信区间[CI]1.45至7.33)、既往卒中史(OR 2.33,95%CI 1.04至5.21)、入院时NIHSS≥18分(OR 2.37,95%CI 1.13至4.99)以及颈内动脉或基底动脉闭塞(OR 2.92,95%CI 1.34至6.40)。利用这些数据,我们制定了用于预测AIS患者接受MT治疗后90天死亡率的(PRACTICE)评分,范围为0至6分。受试者工作特征曲线分析发现,PRACTICE评分(曲线下面积[AUC]=0.744,95%CI 0.669至0.820)在预测90天死亡率方面在数值上优于iScore(AUC=0.661,95%CI 0.577至0.745)和缺血性卒中早期死亡率预测评分(AUC=0.638,95%CI 0.551至0.725)。
我们制定了一个简单的评分系统来估计接受MT治疗的AIS患者的90天死亡率。但该评分系统需要进行前瞻性验证。
中国临床试验注册中心(ChiCTR-OOC-17013052)。