Department of Psychiatry, School of Medicine, Yale University, New Haven, CT, USA.
VA Connecticut Healthcare System, 950 Campbell Ave., Bldg. 36/116A4, West Haven, CT, 06516, USA.
Psychopharmacology (Berl). 2021 Aug;238(8):2083-2090. doi: 10.1007/s00213-021-05833-8. Epub 2021 Apr 1.
Reducing nicotine content of inhaled tobacco products may prevent nicotine addiction, but the threshold for nicotine reinforcement has not been systematically evaluated in controlled human laboratory studies.
The current study uses a novel double-blind placebo-controlled intravenous (IV) nicotine self-administration (NSA) model to determine threshold for subjective effects of nicotine and nicotine reinforcement using a forced choice self-administration procedure.
Young adults (n = 34) had 5 laboratory sessions after overnight nicotine abstinence. In each session, participants sampled and rated the subjective effects of an IV dose of nicotine (0.0125, 0.025, 0.05, 0.1, or 0.2 mg nicotine/70 kg bodyweight) versus saline (placebo), then were given a total of 10 opportunities to self-administer either the IV dose of nicotine or placebo.
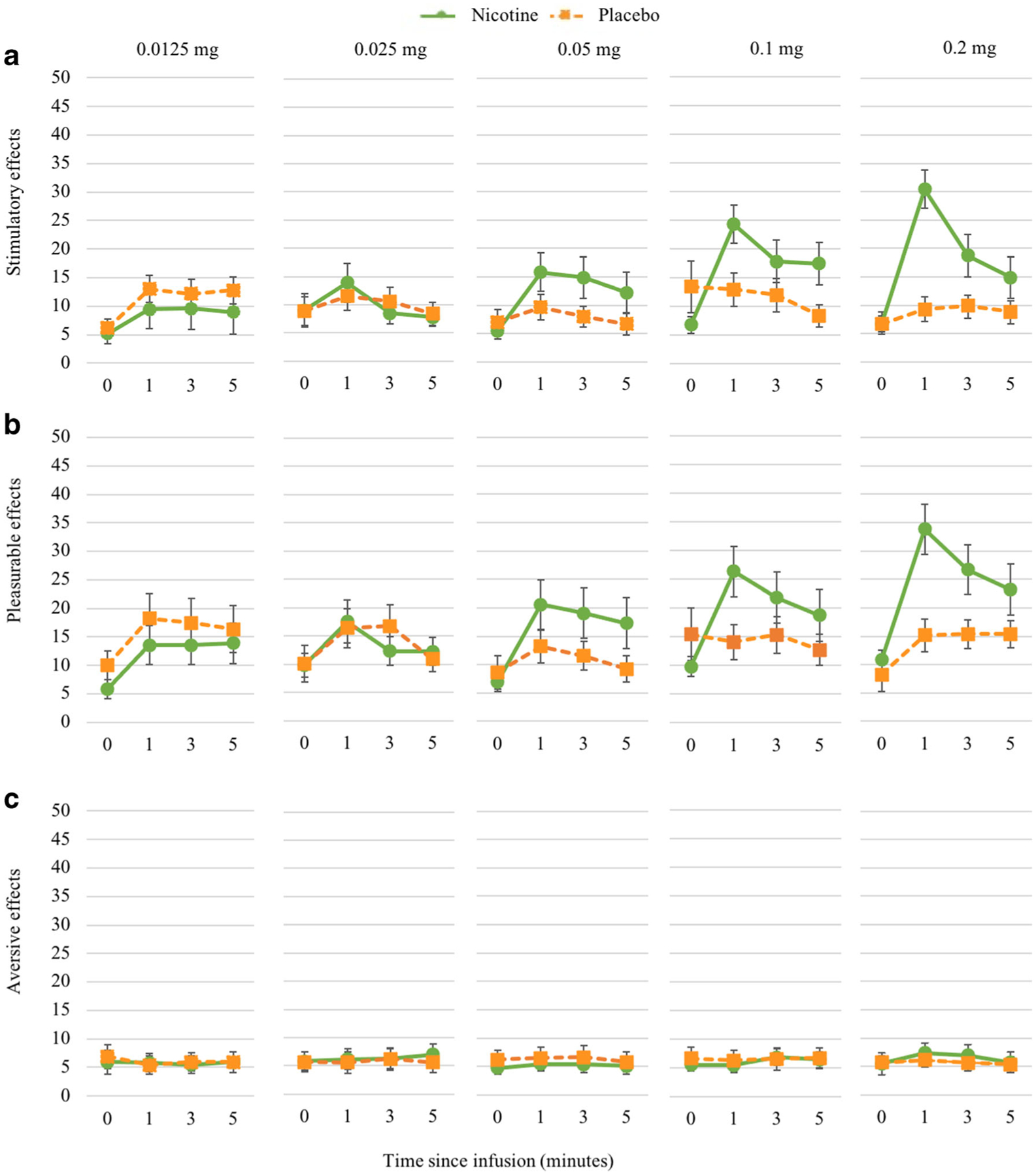
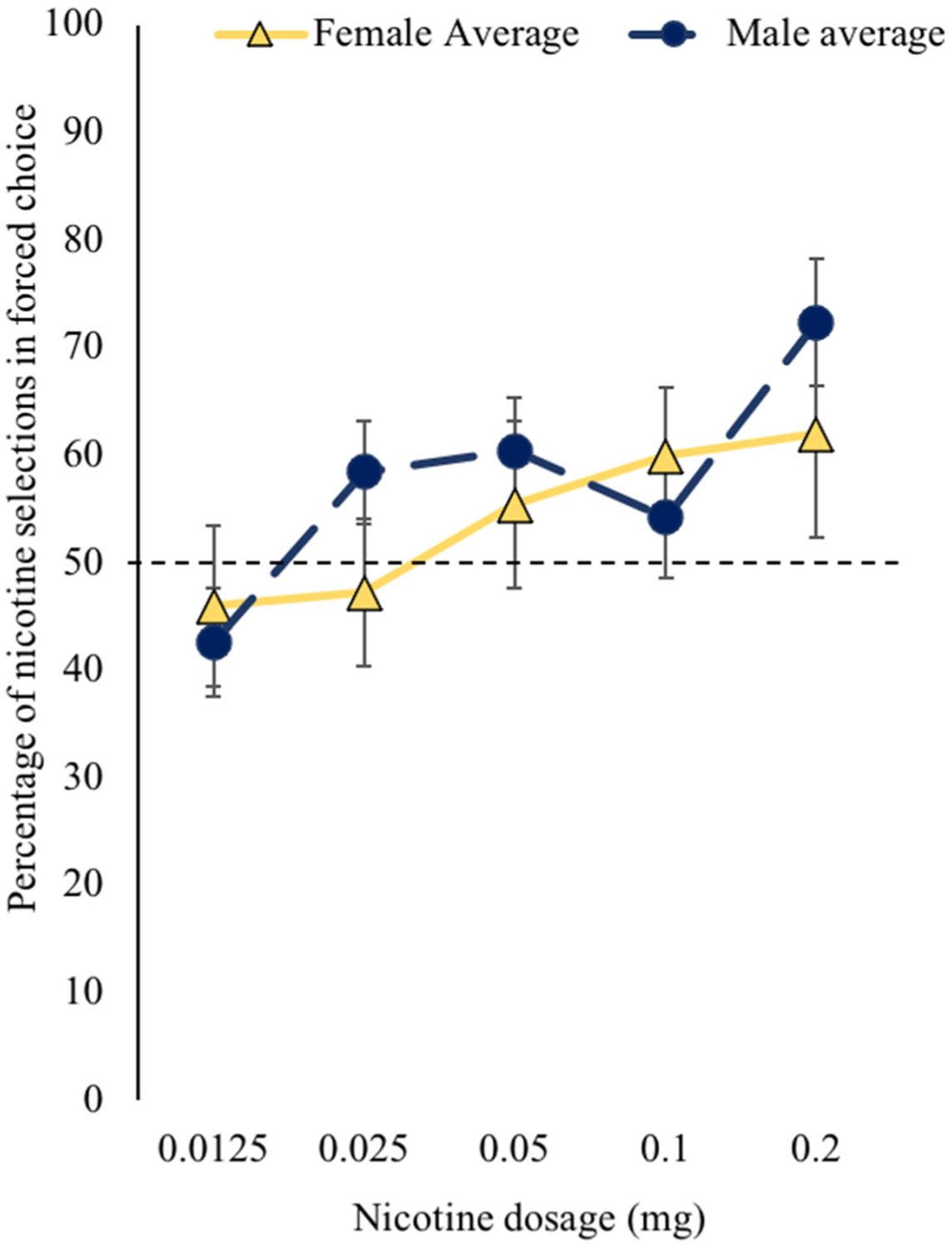
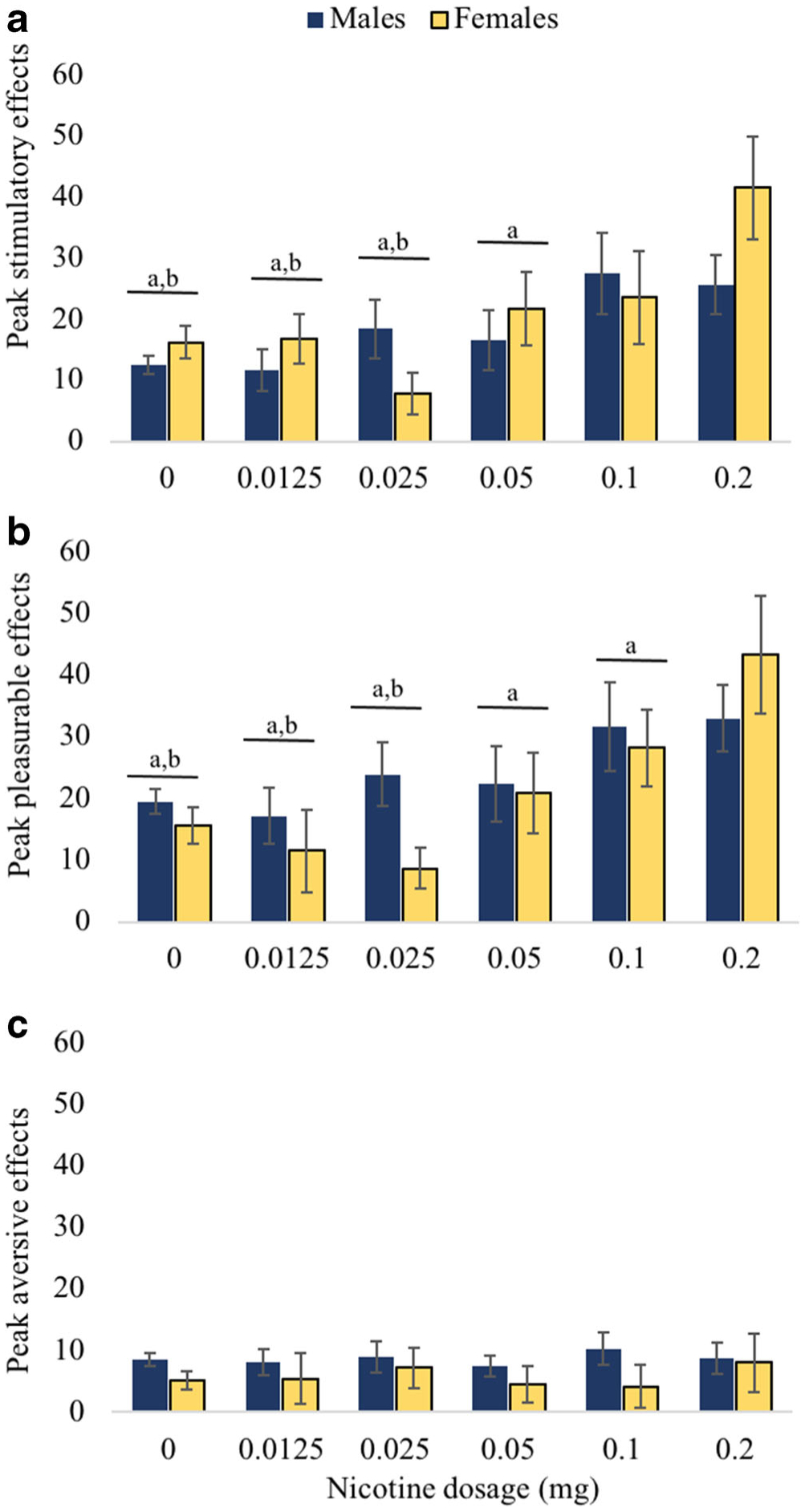
Mixed effect models revealed a significant effect of nicotine dose for positive (i.e., "stimulatory" and "pleasurable"; p < .0001) effects, but not "aversive" effects during sampling period. Post hoc comparisons showed that higher doses (i.e., 0.1 and 0.2 mg) were associated with greater stimulatory, pleasurable, and physiological effects than placebo and lower doses. Mixed effect models revealed that only the highest dose (i.e., 0.2 mg) was consistently preferred over placebo. Sex differences were generally weak (p = .03-.05).
Using our IV nicotine NSA model, the threshold for detecting positive effects of nicotine in young adult smokers is about 0.1 mg, but a higher dose of nicotine, 0.2 mg, is required to produce a consistent nicotine reinforcement. Regarding the regulatory impact, our findings further support the value of nicotine reinforcement threshold as a tobacco regulatory target.
降低吸入式烟草产品中的尼古丁含量可能会预防尼古丁成瘾,但在受控的人体实验室研究中,尚未系统评估尼古丁强化的阈值。
本研究使用一种新颖的双盲安慰剂对照静脉内(IV)尼古丁自我给药(NSA)模型,通过强制选择自我给药程序,确定尼古丁的主观效应和尼古丁强化的阈值。
有吸烟史的年轻成年人(n = 34)在 5 个实验室会议期间经历了一夜的尼古丁戒断。在每个会议中,参与者抽样并评定了 IV 剂量的尼古丁(0.0125、0.025、0.05、0.1 或 0.2 mg 尼古丁/70 kg 体重)与生理盐水(安慰剂)的主观效应,然后总共获得了 10 次自我给予 IV 剂量的尼古丁或安慰剂的机会。
混合效应模型显示,在采样期间,尼古丁剂量对正性(即“兴奋”和“愉悦”)效应有显著影响,但对“厌恶”效应没有影响(p <.0001)。事后比较显示,较高剂量(即 0.1 和 0.2 mg)与安慰剂和较低剂量相比,与更大的兴奋、愉悦和生理效应相关。混合效应模型显示,只有最高剂量(即 0.2 mg)始终比安慰剂更受偏爱。性别差异通常较弱(p =.03-.05)。
使用我们的 IV 尼古丁 NSA 模型,检测年轻成年吸烟者尼古丁正性效应的阈值约为 0.1 mg,但需要更高剂量的尼古丁(0.2 mg)才能产生一致的尼古丁强化作用。关于监管影响,我们的发现进一步支持尼古丁强化阈值作为烟草监管目标的价值。