Martini Nicolò, Testolina Martina, Toffanin Gian Luca, Arancio Rocco, De Mattia Luca, Cannas Sergio, Morani Giovanni, Martini Bortolo
Department of Cardio-Thoraco-Vascular Sciences and Public Health, University of Padua, 35128 Padua, Italy.
Cardiac Unit, Alto Vicentino Hospital, 36014 Santorso, Italy.
J Clin Med. 2021 Mar 2;10(5):1025. doi: 10.3390/jcm10051025.
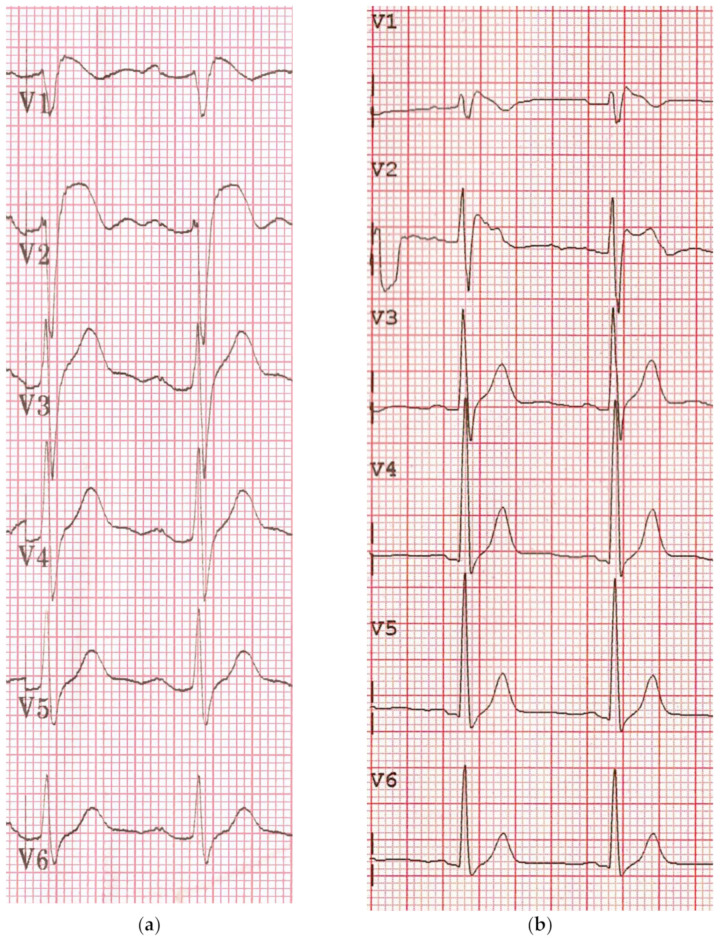
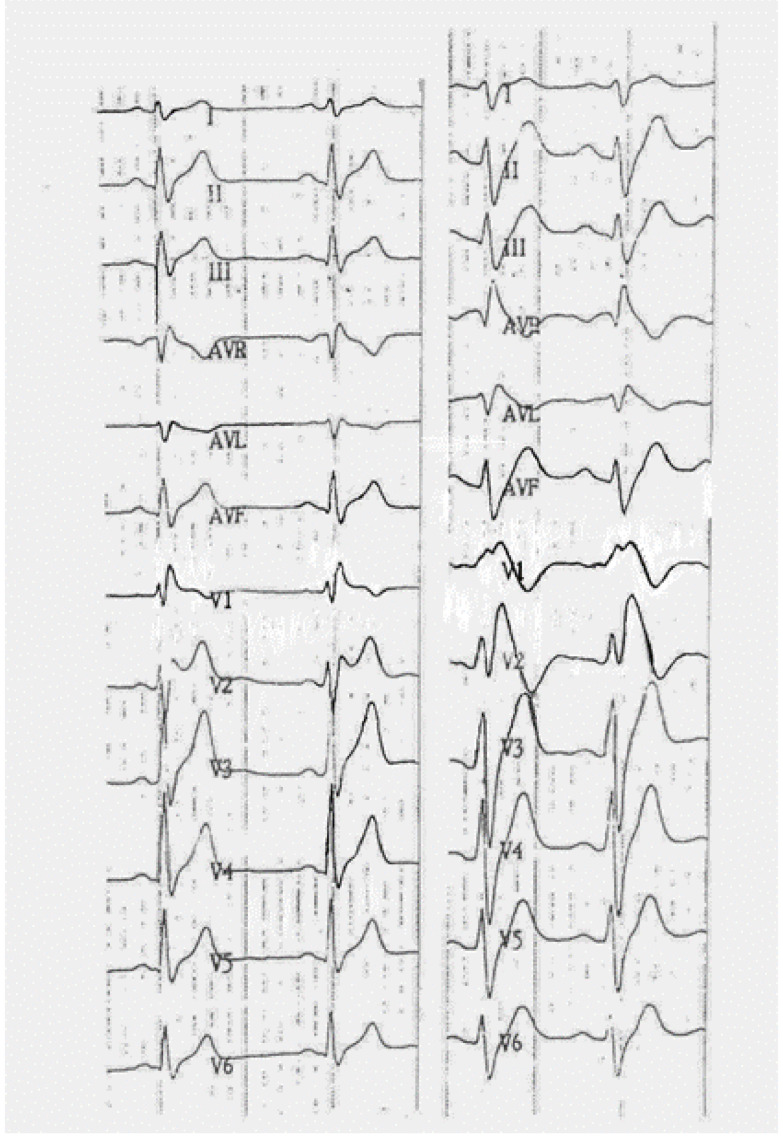
The so-called Brugada syndrome (BS), first called precordial early repolarization syndrome (PERS), is characterized by the association of a fascinating electrocardiographic pattern, namely an aspect resembling right bundle branch block with a coved and sometime upsloping ST segment elevation in the precordial leads, and major ventricular arrhythmic events that could rarely lead to sudden death. Its electrogenesis has been related to a conduction delay mostly, but not only, located on the right ventricular outflow tract (RVOT), probably due to a progressive fibrosis of the conduction system. Many tests have been proposed to identify people at risk of sudden death and, among all, ajmaline challenge, thanks to its ability to enhance latent conduction defects, became so popular, even if its role is still controversial as it is neither specific nor sensitive enough to guide further invasive investigations and managements. Interestingly, a type 1 pattern has also been induced in many other cardiac diseases or systemic diseases with a cardiac involvement, such as long QT syndrome (LQTS), arrhythmogenic right ventricular cardiomyopathy (ARVC), hypertrophic cardiomyopathy (HCM) and myotonic dystrophy, without any clear arrhythmic risk profile. Evidence-based studies clearly showed that a positive ajmaline test does not provide any additional information on the risk stratification for major ventricular arrhythmic events on asymptomatic individuals with a non-diagnostic Brugada ECG pattern.
所谓的Brugada综合征(BS),最初被称为心前区早期复极综合征(PERS),其特征是伴有一种引人注目的心电图模式,即类似右束支传导阻滞的表现,心前区导联出现下斜型且有时呈上斜型的ST段抬高,以及可能很少导致猝死的严重室性心律失常事件。其电生理机制主要与传导延迟有关,这种传导延迟大多(但并非仅)位于右心室流出道(RVOT),可能是由于传导系统的进行性纤维化所致。已经提出了许多检测方法来识别猝死风险人群,其中,阿义马林激发试验因其能够增强潜在的传导缺陷而变得非常流行,尽管其作用仍存在争议,因为它既不够特异也不够敏感,无法指导进一步的侵入性检查和治疗。有趣的是,在许多其他伴有心脏受累的心脏疾病或全身性疾病中,如长QT综合征(LQTS)、致心律失常性右室心肌病(ARVC)、肥厚型心肌病(HCM)和强直性肌营养不良,也可诱发1型心电图模式,但没有任何明确的心律失常风险特征。循证研究清楚地表明,对于心电图表现不典型的无症状个体,阿义马林激发试验阳性并不能为严重室性心律失常事件的风险分层提供任何额外信息。