Department of Cardiology and Internal Medicine, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, 85-094 Bydgoszcz, Poland.
Division of Cardiovascular Medicine, University of California San Diego, La Jolla, CA 92037, USA.
Int J Mol Sci. 2021 Mar 20;22(6):3169. doi: 10.3390/ijms22063169.
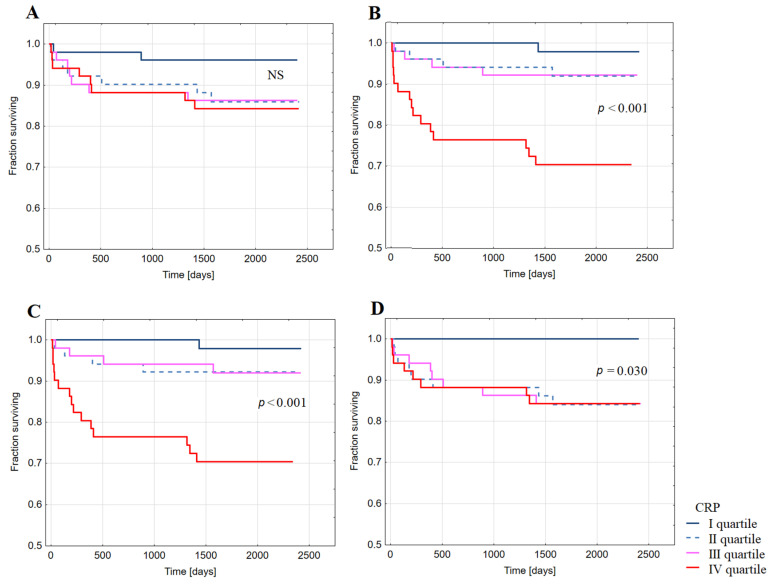
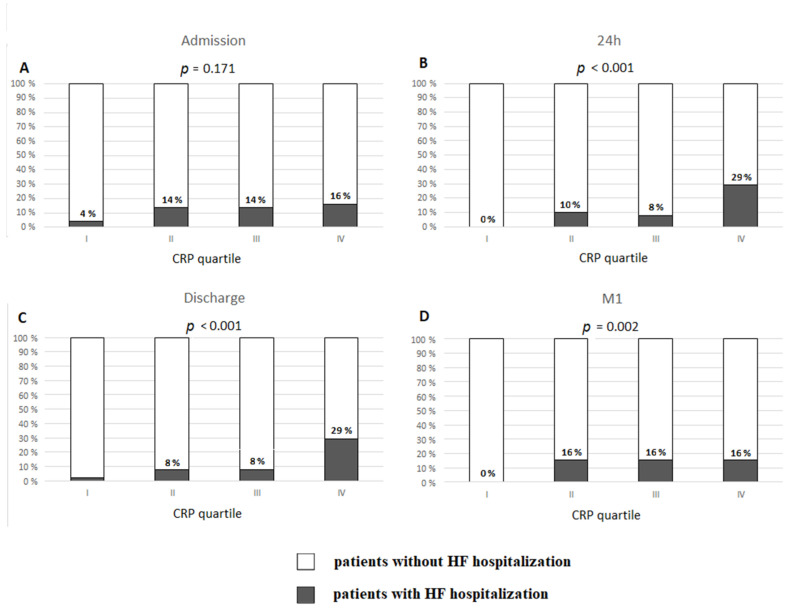
Inflammatory activation during acute ST-elevation myocardial infarction (STEMI) can contribute to post-infarct heart failure (HF). This study aimed to determine prognostic value of high-sensitivity C-reactive protein concentration (CRP) for HF over a long-term follow-up in 204 patients with a first STEMI undergoing guideline-based therapies including percutaneous coronary intervention. CRP was measured at admission, 24 h (CRP), discharge (CRP), and one month (CRP) after index hospitalization for STEMI. Within a median period of 5.6 years post-index hospitalization for STEMI, hospitalization for HF (HFH) which is a primary endpoint, occurred in 24 patients (11.8%, HF+ group). During the study, 8.3% of HF+ patients died vs. 1.7% of patients without HFH (HF- group) ( = 0.047). CRP, CRP, and CRP were significantly higher in HF+ compared to HF- group. The median CRP in HF+ group was 2.57 mg/L indicating low-grade systemic inflammation, in contrast to 1.54 mg/L in HF- group. CRP ≥ 2 mg/L occurred in 58.3% of HF+ vs. 42.8% of HF- group ( = 0.01). Kaplan-Meier analysis showed decreased probability of survival free from HFH in patients with CRP ( < 0.001), CRP ( < 0.001), and CRP ( = 0.03) in quartile IV compared to lower quartiles. In multivariable analysis, CRP significantly improved prediction of HFH over a multi-year period post-STEMI. Persistent elevation in CRP post STEMI aids in risk stratification for long-term HF and suggests that ongoing cardiac and low-grade systemic inflammation promote HF development despite guideline-based therapies.
在急性 ST 段抬高型心肌梗死(STEMI)期间的炎症激活可导致梗死后心力衰竭(HF)。本研究旨在确定在接受包括经皮冠状动脉介入治疗在内的指南指导治疗的 204 例首次 STEMI 患者中,高敏 C 反应蛋白浓度(CRP)在长期随访中的 HF 预后价值。在 STEMI 指数住院期间,在入院时(CRP)、24 小时(CRP)、出院时(CRP)和一个月(CRP)测量 CRP。在 STEMI 指数住院后中位 5.6 年内,因 HF 住院(HFH)作为主要终点,24 例患者(11.8%,HF+组)发生。在研究期间,HF+组中有 8.3%的患者死亡,而无 HFH 的患者(HF-组)有 1.7%死亡(= 0.047)。HF+组的 CRP、CRP 和 CRP 均显著高于 HF-组。HF+组的 CRP 中位数为 2.57mg/L,表明存在低度全身性炎症,而 HF-组为 1.54mg/L。HF+组中 CRP≥2mg/L 的发生率为 58.3%,而 HF-组为 42.8%(= 0.01)。Kaplan-Meier 分析显示,与 CRP 较低四分位数的患者相比,CRP(<0.001)、CRP(<0.001)和 CRP(= 0.03)四分位 IV 的患者 HFH 无生存概率降低。多变量分析显示,CRP 可显著改善 STEMI 后多年 HF 的预测。STEMI 后 CRP 持续升高有助于对长期 HF 进行风险分层,并表明尽管进行了指南指导的治疗,但持续的心脏和低度全身性炎症仍会促进 HF 的发生。