Shaffer Jeffrey G, Schieffelin John S, Momoh Mambu, Goba Augustine, Kanneh Lansana, Alhasan Foday, Gbakie Michael, Engel Emily J, Bond Nell G, Hartnett Jessica N, Nelson Diana K S, Bush Duane J, Boisen Matthew L, Heinrich Megan L, Rowland Megan M, Branco Luis M, Samuels Robert J, Garry Robert F, Grant Donald S
Department of Biostatistics and Data Science, School of Public Health and Tropical Medicine, Tulane University, New Orleans, LA 70112, USA.
Sections of Infectious Disease, Departments of Pediatrics and Internal Medicine, School of Medicine, Tulane University, New Orleans, LA 70112, USA.
Microorganisms. 2021 Mar 12;9(3):586. doi: 10.3390/microorganisms9030586.
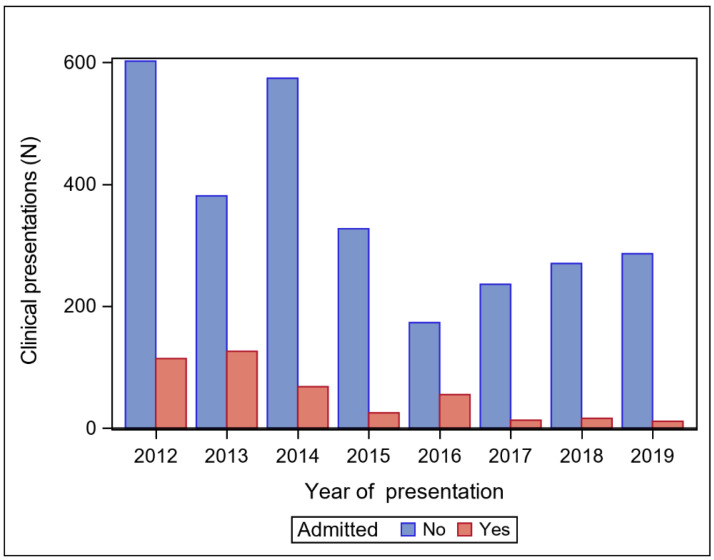
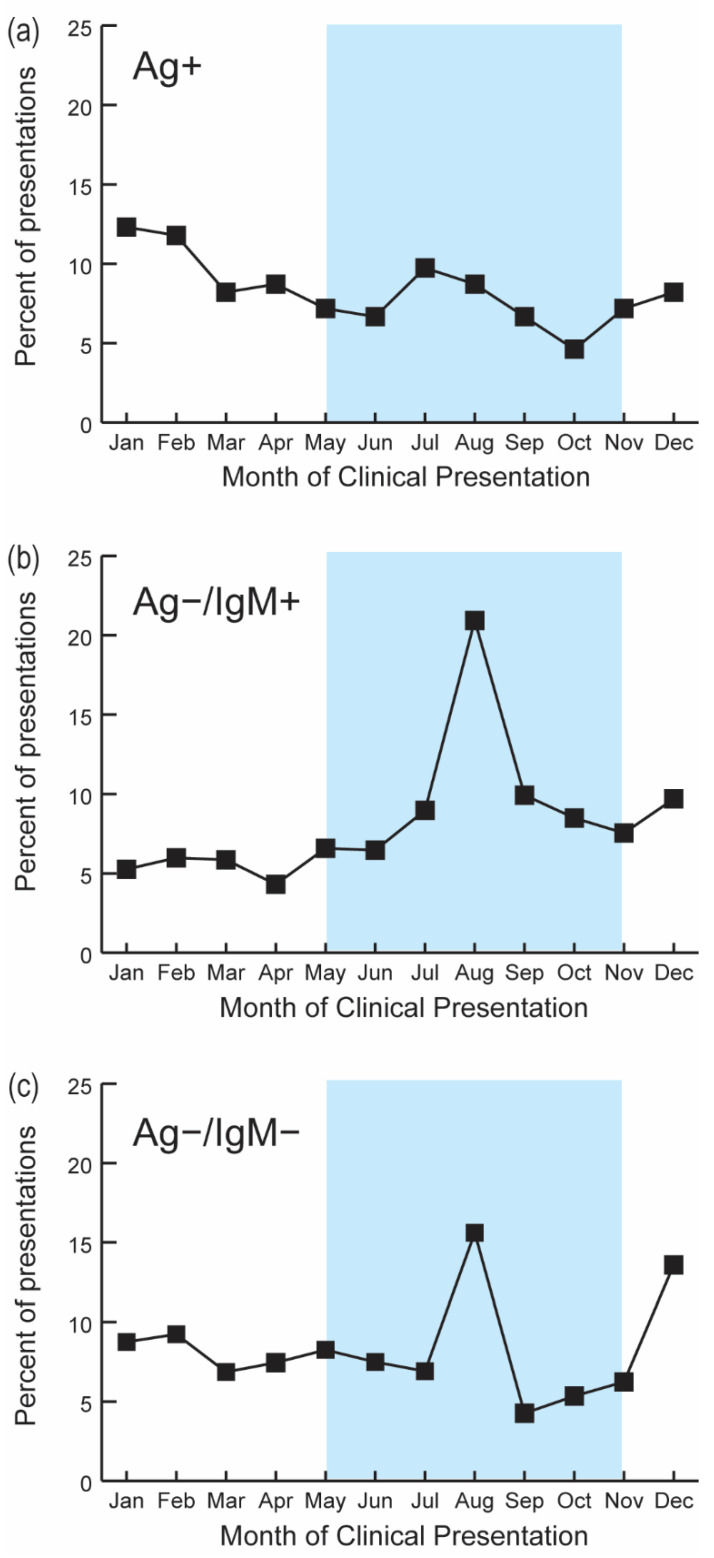
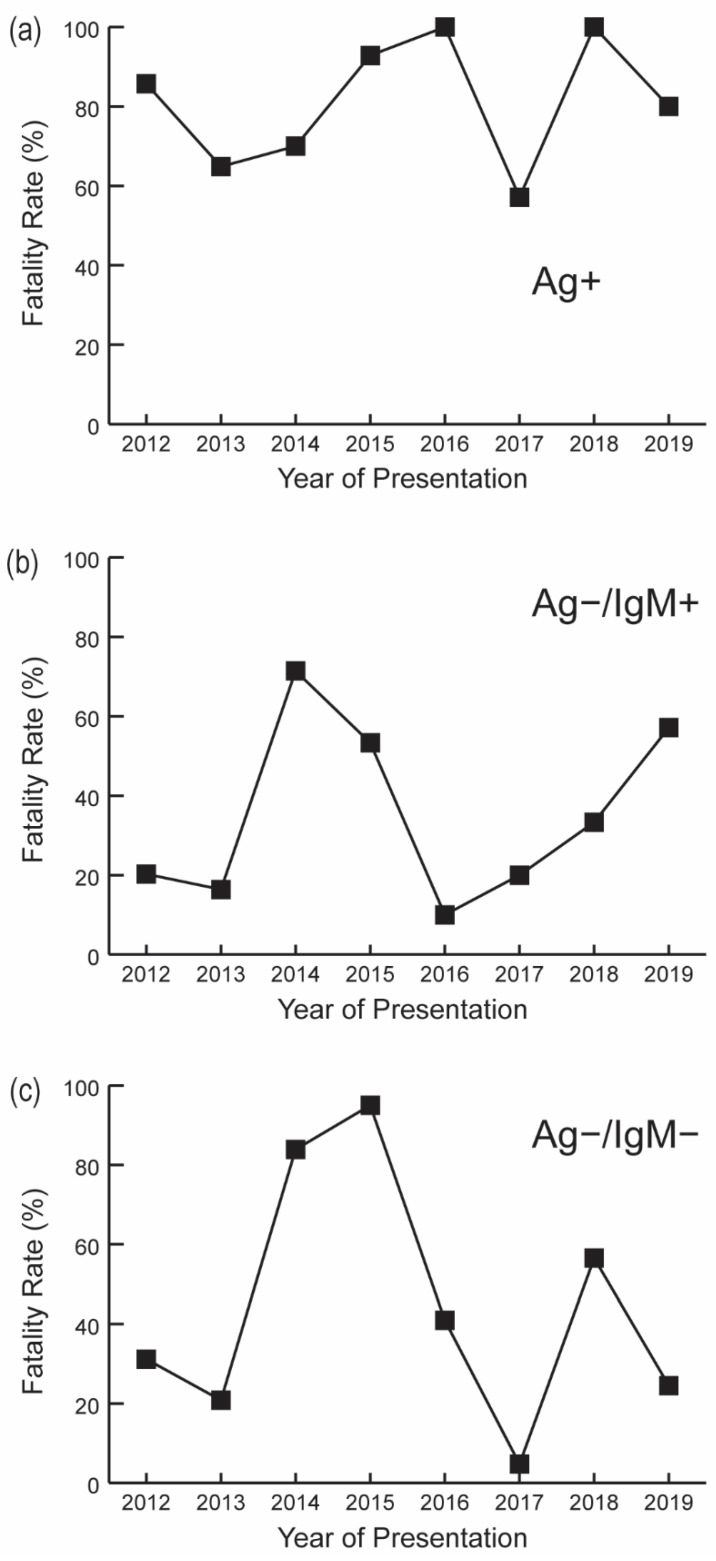
Lassa fever (LF) is a viral hemorrhagic disease found in Sub-Saharan Africa and is responsible for up to 300,000 cases and 5000 deaths annually. LF is highly endemic in Sierra Leone, particularly in its Eastern Province. Kenema Government Hospital (KGH) maintains one of only a few LF isolation facilities in the world with year-round diagnostic testing. Here we focus on space-time trends for LF occurring in Sierra Leone between 2012 and 2019 to provide a current account of LF in the wake of the 2014-2016 Ebola epidemic. Data were analyzed for 3277 suspected LF cases and classified as acute, recent, and non-LF or prior LF exposure using enzyme-linked immunosorbent assays (ELISAs). Presentation rates for acute, recent, and non-LF or prior LF exposure were 6.0% (195/3277), 25.6% (838/3277), and 68.4% (2244/3277), respectively. Among 2051 non-LF or prior LF exposures, 33.2% (682/2051) tested positive for convalescent LF exposure. The overall LF case-fatality rate (CFR) was 78.5% (106/135). Both clinical presentations and confirmed LF cases declined following the Ebola epidemic. These declines coincided with an increased duration between illness onset and clinical presentation, perhaps suggesting more severe disease or presentation at later stages of illness. Acute LF cases and their corresponding CFRs peaked during the dry season (November to April). Subjects with recent (but not acute) LF exposure were more likely to present during the rainy season (May to October) than the dry season ( < 0.001). The findings here suggest that LF remains endemic in Sierra Leone and that caseloads are likely to resume at levels observed prior to the Ebola epidemic. The results provide insight on the current epidemiological profile of LF in Sierra Leone to facilitate LF vaccine studies and accentuate the need for LF cohort studies and continued advancements in LF diagnostics.
拉沙热(LF)是一种在撒哈拉以南非洲发现的病毒性出血热疾病,每年导致多达30万例病例和5000人死亡。拉沙热在塞拉利昂高度流行,尤其是在其东部省份。凯内马政府医院(KGH)是世界上仅有的少数几个常年进行诊断检测的拉沙热隔离设施之一。在此,我们关注2012年至2019年期间塞拉利昂发生的拉沙热的时空趋势,以便在2014 - 2016年埃博拉疫情之后提供拉沙热的最新情况。对3277例疑似拉沙热病例的数据进行了分析,并使用酶联免疫吸附测定(ELISA)将其分类为急性、近期感染以及非拉沙热或既往拉沙热暴露。急性、近期感染以及非拉沙热或既往拉沙热暴露的就诊率分别为6.0%(195/3277)、25.6%(838/3277)和68.4%(2244/3277)。在2051例非拉沙热或既往拉沙热暴露病例中,33.2%(682/2051)恢复期拉沙热暴露检测呈阳性。拉沙热总体病死率(CFR)为78.5%(106/135)。埃博拉疫情之后,临床症状表现和确诊的拉沙热病例均有所下降。这些下降与发病至临床症状出现之间的时间延长相吻合,这可能表明病情更严重或在疾病后期才出现症状。急性拉沙热病例及其相应的病死率在旱季(11月至4月)达到峰值。近期(但非急性)感染拉沙热的患者在雨季(5月至10月)就诊的可能性高于旱季(<0.001)。此处的研究结果表明,拉沙热在塞拉利昂仍然流行,病例数可能会恢复到埃博拉疫情之前观察到的水平。这些结果为塞拉利昂拉沙热当前的流行病学概况提供了见解,以促进拉沙热疫苗研究,并强调开展拉沙热队列研究以及持续推进拉沙热诊断技术的必要性。