Illum Benjamin, Odish Mazen, Minokadeh Anushirvan, Yi Cassia, Owens Robert L, Pollema Travis, LaBuzetta Jamie Nicole
Department of Neurosciences, Division of Neurocritical Care, La Jolla, USA.
Department of Medicine, Division of Pulmonary, Critical Care, and Sleep Medicine, 9300 Campus Point Drive Mail Code #7381, La Jolla, CA 92037-7381 USA.
Curr Treat Options Neurol. 2021;23(5):15. doi: 10.1007/s11940-021-00671-7. Epub 2021 Mar 31.
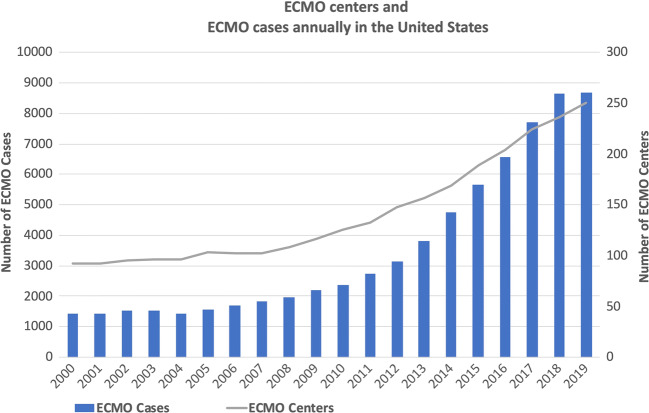
Extracorporeal membrane oxygen (ECMO) is increasingly used as an advanced form of life support for cardiac and respiratory failure. Unfortunately, in infrequent instances, circulatory and/or respiratory recovery is overshadowed by neurologic injury that can occur in patients who require ECMO. As such, knowledge of ECMO and its implications on diagnosis and treatment of neurologic injuries is indispensable for intensivists and neurospecialists.
The most common neurologic injuries include intracerebral hemorrhage, ischemic stroke, seizure, cerebral edema, intracranial hypertension, global cerebral hypoxia/anoxia, and brain death. These result from events prior to initiation of ECMO, failure of ECMO to provide adequate oxygen delivery, and/or complications that occur during ECMO. ECMO survivors also experience neurological and psychological sequelae similar to other survivors of critical illness.
Since many of the risk factors for neurologic injury cannot be easily mitigated, early diagnosis and intervention are crucial to limit morbidity and mortality from neurologic injury during ECMO.
体外膜肺氧合(ECMO)越来越多地被用作治疗心脏和呼吸衰竭的一种高级生命支持形式。不幸的是,在少数情况下,需要ECMO的患者可能会出现神经损伤,从而使循环和/或呼吸功能的恢复黯然失色。因此,对于重症监护医生和神经专科医生来说,了解ECMO及其对神经损伤诊断和治疗的影响是必不可少的。
最常见的神经损伤包括脑出血、缺血性中风、癫痫发作、脑水肿、颅内高压、全脑缺氧/缺血以及脑死亡。这些损伤是由ECMO启动前的事件、ECMO未能提供足够的氧输送和/或ECMO期间发生的并发症导致的。ECMO幸存者还会经历与其他危重病幸存者类似的神经和心理后遗症。
由于许多神经损伤的危险因素难以轻易缓解,早期诊断和干预对于限制ECMO期间神经损伤的发病率和死亡率至关重要。