Aljehani Yasser, Othman Sharifah A, Almubarak Yousif, Elbaz Ayman, Sabry Mohammed, Alreshaid Farouk, Elbawab Hatem Y, Alghamdi Zeead M, Alshahrani Mohammed
Division of Thoracic Surgery, Department of Surgery, King Fahad Hospital of the University, Khobar, Saudi Arabia.
College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
Crit Care Res Pract. 2021 Mar 27;2021:6626150. doi: 10.1155/2021/6626150. eCollection 2021.
Iatrogenic pneumothoracis, barotraumas, and tracheoesophageal fistulae, especially after prolonged intubation, and tracheal stenosis are all entities involving thoracic surgeons' consultation and management. With the surge of COVID-19 cases particularly in the critical care settings, various types of complications have been observed that require intervention from thoracic surgeons.
A retrospective study was conducted in an academic healthcare institute in the Eastern Province of Saudi Arabia. We included all COVID-19 cases admitted to ICU in the period between March 15, 2020, and August 15, 2020, requiring thoracic surgery consultation and management. Non-COVID-19 critical cases and iatrogenic pneumothorax were excluded.
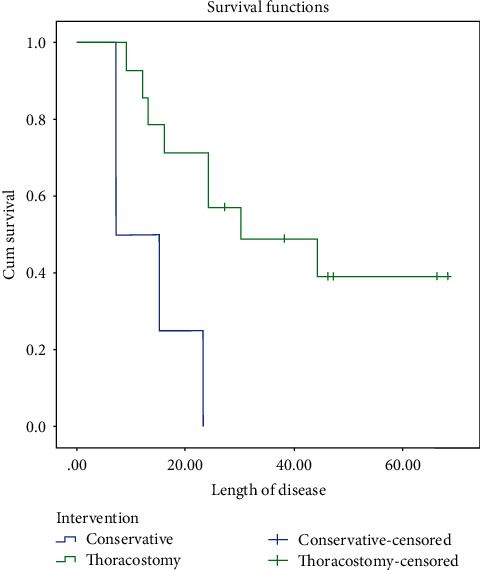
Of 122 patients who were admitted to ICU with COVID-19, 18 patients (14.75%) required thoracic surgery consultation and management. We discovered a significant association between the outcomes and reintubation rates and the rate of pneumothorax occurrence. The survival analysis showed improvement in patients who had thoracostomy tube insertion as a management than the group who were treated conservatively. On the other hand, there was a significant difference between the COVID ICU group who had thoracic complication and those who did not regarding the length of hospital stay.
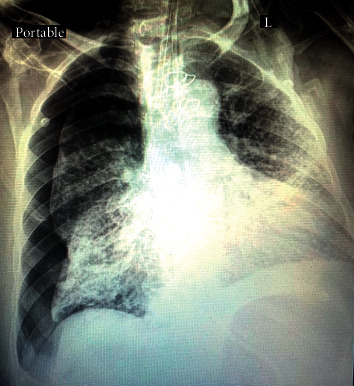
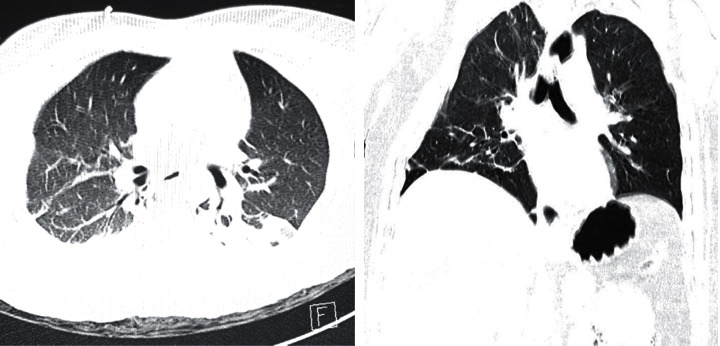
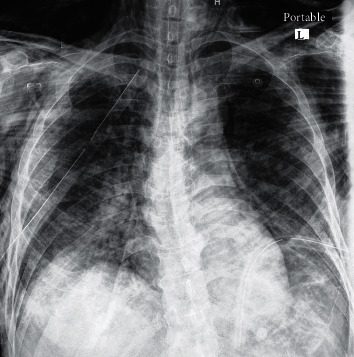
Noniatrogenic pneumothorax, subcutaneous emphysema, and mediastinal emphysema are well-known thoracic entities, but their presence in the context of COVID-19 disease is a harbinger for worse prognosis and outcomes. The presence of pneumothorax may be associated with better prognosis and outcome compared to surgical and mediastinal emphysema.
医源性气胸、气压伤和气管食管瘘,尤其是长期插管后出现的情况,以及气管狭窄,均属于需要胸外科医生会诊和处理的病症。随着新型冠状病毒肺炎(COVID-19)病例的激增,尤其是在重症监护环境中,已观察到各种需要胸外科医生干预的并发症。
在沙特阿拉伯东部省份的一家学术性医疗机构进行了一项回顾性研究。我们纳入了2020年3月15日至2020年8月15日期间入住重症监护病房(ICU)且需要胸外科会诊和处理的所有COVID-19病例。排除非COVID-19重症病例和医源性气胸病例。
在122例因COVID-19入住ICU的患者中,18例(14.75%)需要胸外科会诊和处理。我们发现结局和再次插管率与气胸发生率之间存在显著关联。生存分析表明,接受胸腔造瘘管置入治疗的患者比保守治疗的患者情况有所改善。另一方面,发生胸部并发症的COVID-19 ICU组与未发生并发症的组在住院时间方面存在显著差异。
非医源性气胸、皮下气肿和纵隔气肿是常见的胸部病症,但在COVID-19疾病背景下出现这些情况预示着预后和结局较差。与手术性气肿和纵隔气肿相比,气胸的存在可能与较好的预后和结局相关。