Aljehani Yasser, Alkhunaizi Auday A, Othman Sharifah A, Alqumber Hassan Abdullah, Almubarak Yousif, Al-Musawi Tariq, Al Bazroun Mohammed Ibrahim, Alshaikhmohamed Khatoon
Division of Thoracic Surgery, Department of Surgery, King Fahad Hospital of the University, College of Medicine, Imam Abdulrahman Bin Faisal University, Damam, Saudi Arabia.
Department of Emergency Medicine, Qatif Central Hospital, Qatif, Saudi Arabia.
Ann Thorac Med. 2022 Jan-Mar;17(1):51-58. doi: 10.4103/atm.atm_600_20. Epub 2022 Jan 14.
Coronavirus illness 2019, commonly referred to as COVID-19, is a highly infectious disease brought on by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). COVID-19 was declared a universal pandemic in March 2020 by the World Health Organization and is a severe health issue with unprecedented morbidity and mortality rates. Both surgical and mediastinal emphysema have been seen in cases of critically ill COVID-19 patients in several hospitals in the Eastern Province of Saudi Arabia.
This was a retrospective, cross-sectional, multicentric study involving several hospitals in the Saudi Arabian Eastern Province. Data were collected from intensive care units (ICUs) in these hospitals from March 2 to August 2, 2020. The inclusion criteria consisted of all patients who tested positive for SARS-CoV-2 and were admitted to a critical care unit.
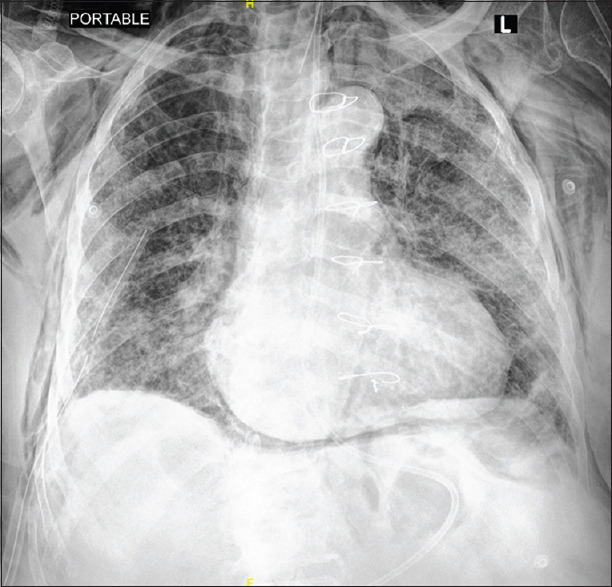
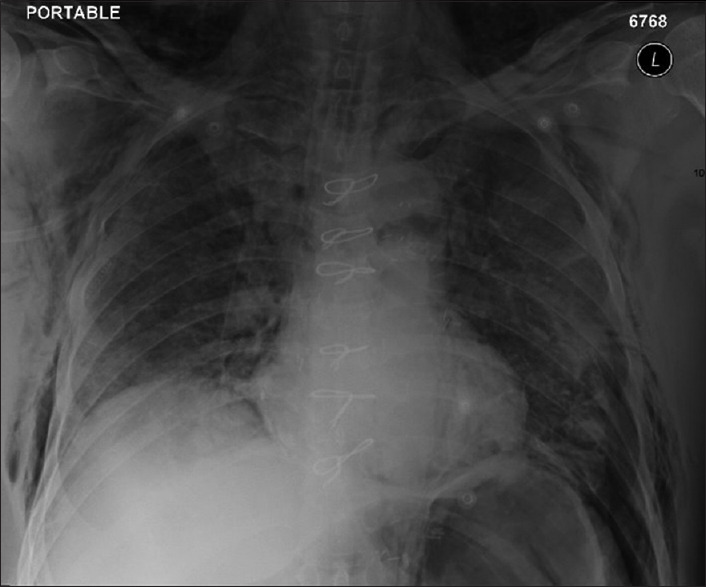
Thirty patients required thoracic consultation and management, including 26 males (81.3%) and 4 females (12.5%) (1:0.15) who developed surgical and mediastinal emphysema requiring thoracic surgery intervention. Most of the patients were on high ventilation settings, and the mean duration of ventilator support was 16.50 ± 13.98 days. Two patients (6.3%) required reintubation. The median positive end-expiratory pressure (PEEP) was 12 ± 2.80 cmHO with a median FiO2 of 70% ± 19.73. On average, thoracic complications occurred on day 3 (±6.29 days) postintubation. Ten patients (33.33%) experienced a pneumothorax associated with surgical emphysema (SE), 1 patient (3.33%) presented with only mediastinal emphysema; 17 patients (56.66%) with only SE, and 1 (3.33%) had mediastinal emphysema associated with SE. We noted a correlation between the duration of ventilator support, the length of ICU stay ( < 0.001), and the total length of stay (LOS) in the hospital ( < 0.001). Total length of hospital stay showed significant association with the onset of complications ( = 0.045) and outcomes ( = 0.006). A significant association between PEEP and the duration of ventilator support was also evident with a value = 0.009 and the onset of complications ( = 0.043). In addition, we found a significant association between the group with pneumothorax in combination with SE, and their outcomes, with a = 0.002.
Surgical and mediastinal emphysema in the critically ill patients are usually attributed to barotrauma and high ventilations settings. During COVID-19 pandemic, these entities were seen and the pathogenesis was revisited and some attributed its presence to the disease process and destruction on lung parenchyma. The associated with extended LOS and delayed recovery in addition to poor prognosis were seen. Their presence is an indicator to higher morbidity and mortality.
2019年冠状病毒病,通常称为COVID-19,是由严重急性呼吸综合征冠状病毒2(SARS-CoV-2)引起的一种高度传染性疾病。2020年3月,世界卫生组织宣布COVID-19为全球大流行疾病,它是一个严重的健康问题,发病率和死亡率空前。沙特阿拉伯东部省份的几家医院在重症COVID-19患者病例中均观察到手术性肺气肿和纵隔气肿。
这是一项回顾性、横断面、多中心研究,涉及沙特阿拉伯东部省份的几家医院。数据收集自2020年3月2日至8月2日这些医院的重症监护病房(ICU)。纳入标准包括所有SARS-CoV-2检测呈阳性并入住重症监护病房的患者。
30例患者需要胸科会诊和治疗,其中26例男性(81.3%)和4例女性(12.5%)(比例为1:0.15)发生了需要胸外科手术干预的手术性肺气肿和纵隔气肿。大多数患者处于高通气设置,呼吸机支持的平均时长为16.50±13.98天。2例患者(6.3%)需要再次插管。呼气末正压(PEEP)的中位数为12±2.80 cmH₂O,吸入氧浓度(FiO₂)的中位数为70%±19.73。平均而言,胸科并发症在插管后第3天(±6.29天)出现。10例患者(33.33%)发生了与手术性肺气肿(SE)相关的气胸,1例患者(3.33%)仅表现为纵隔气肿;17例患者(56.66%)仅有SE,1例(3.33%)有与SE相关的纵隔气肿。我们注意到呼吸机支持时长、ICU住院时长(<0.001)以及医院总住院时长(LOS)之间存在相关性(<0.001)。医院总住院时长与并发症的发生(=0.045)和结局(=0.006)显示出显著相关性。PEEP与呼吸机支持时长之间也存在显著相关性,值为0.009,与并发症的发生(=0.043)也相关。此外,我们发现气胸合并SE组与其结局之间存在显著相关性,=0.002。
重症患者的手术性肺气肿和纵隔气肿通常归因于气压伤和高通气设置。在COVID-19大流行期间,观察到了这些情况,对其发病机制进行了重新审视,一些人将其存在归因于疾病过程和肺实质的破坏。除了预后不良外,还观察到其与延长的住院时长和恢复延迟相关。它们的存在是更高发病率和死亡率的一个指标。