Department of Emergency Medicine, University of Ulsan College of Medicine, Asan Medical Center, 88, Olympic-ro 43-gil., Songpa-gu, Seoul, 05505, Korea.
Crit Care. 2021 Jan 6;25(1):11. doi: 10.1186/s13054-020-03421-4.
We evaluated the characteristics and outcomes of culture-negative versus culture-positive septic shock.
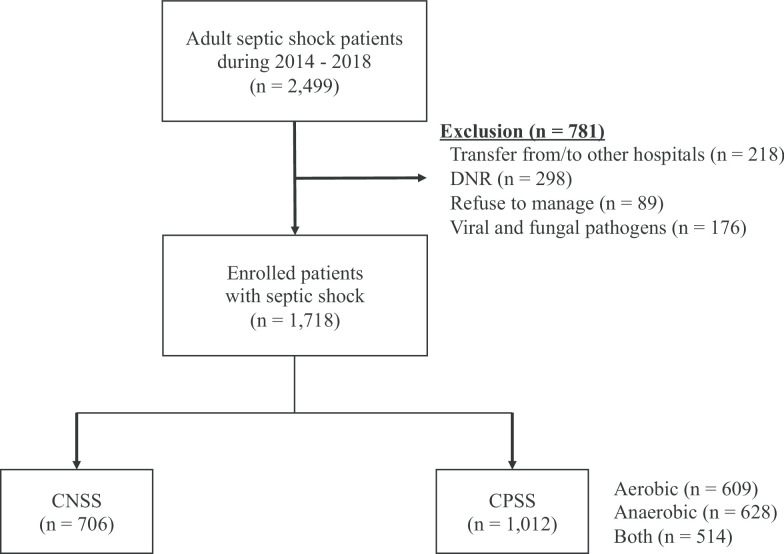
We performed a retrospective observational study of data from a prospective registry from 2014 to 2018. A total of 2,499 adult patients with septic shock were enrolled. The primary outcome was 90-day mortality, and the secondary outcomes were the length of hospital stay, a requirement for mechanical ventilation or renal replacement therapy, and in-hospital mortality.
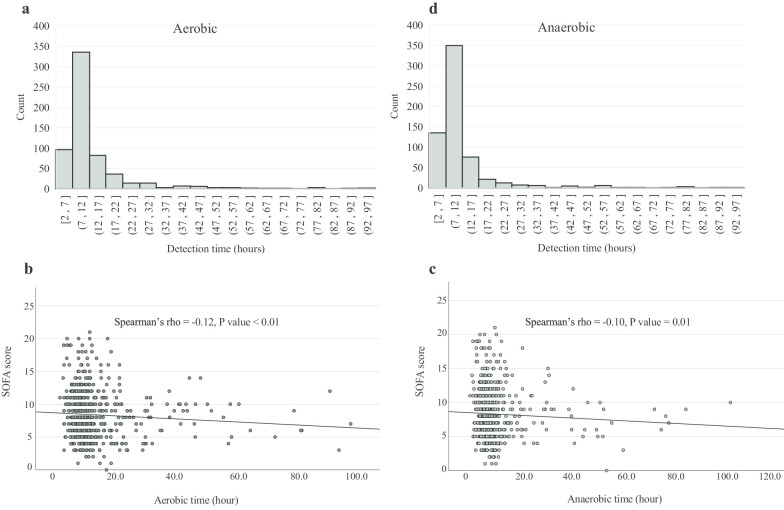
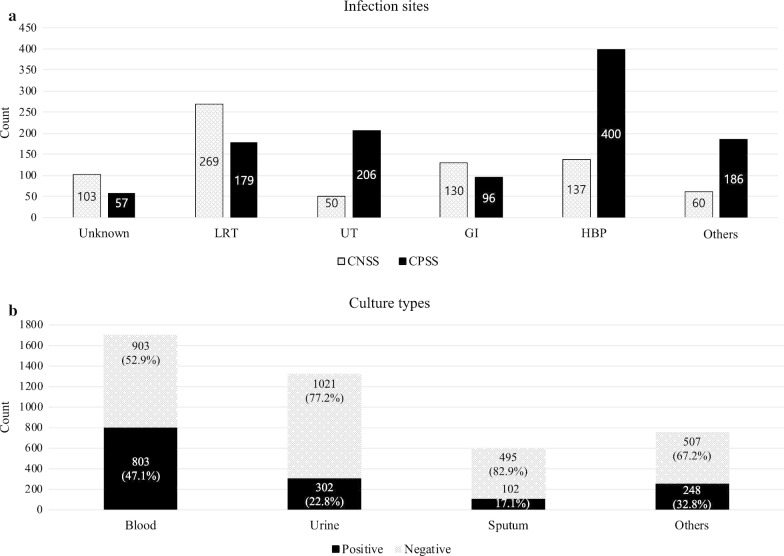
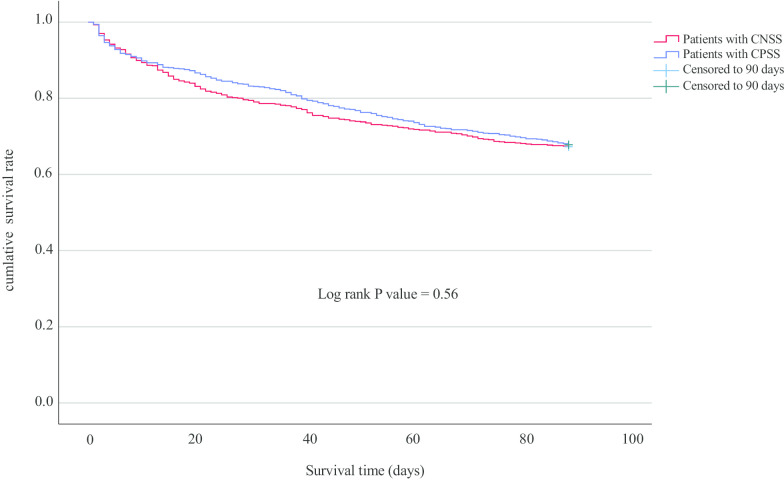
Of 1,718 patients with septic shock, 1,012 (58.9%) patients were culture-positive (blood 803, urine 302, sputum 102, others 204) and the median pathogen detection time was 9.5 h (aerobic 10.2 h and anaerobic 9.0 h). The most common site of culture-positive infection was the hepatobiliary tract (39.5%), while for the culture-negative it was the lower respiratory tract (38.2%). The culture-negative group had a lower mean body temperature (37.3 vs 37.7 ℃), lactate (2.5 vs. 3.2 mmol/L), C-reactive protein (11.1 vs 11.9 mg/dL), and sequential organ failure assessment score (7.0 vs. 8.0) than that of the culture-positive group. However, 90-day mortality between the groups was not significantly different (32.7 vs 32.2%, p = 0.83), and the other clinical outcomes also did not differ significantly. Moreover, a shorter culture detection time was correlated with a higher sequential organ failure assessment score but not with mortality.
Patients with septic shock are frequently culture-negative, especially in cases where the infection focus is in the lower respiratory tract. Although culture-negative was associated with a degree of organ dysfunction, it was not an independent predictor of death.
我们评估了培养阴性与培养阳性感染性休克的特征和结局。
我们对 2014 年至 2018 年前瞻性登记研究的数据进行了回顾性观察研究。共纳入 2499 例成人感染性休克患者。主要结局为 90 天死亡率,次要结局为住院时间、机械通气或肾脏替代治疗的需求以及院内死亡率。
在 1718 例感染性休克患者中,1012 例(58.9%)为培养阳性(血 803 例,尿 302 例,痰 102 例,其他部位 204 例),中位病原体检测时间为 9.5 小时(需氧菌 10.2 小时,厌氧菌 9.0 小时)。培养阳性感染最常见的部位是肝胆系统(39.5%),而培养阴性感染最常见的部位是下呼吸道(38.2%)。培养阴性组的平均体温(37.3℃比 37.7℃)、乳酸(2.5mmol/L 比 3.2mmol/L)、C 反应蛋白(11.1mg/dL 比 11.9mg/dL)和序贯器官衰竭评估评分(7.0 分比 8.0 分)均低于培养阳性组。然而,两组 90 天死亡率无显著差异(32.7%比 32.2%,p=0.83),其他临床结局也无显著差异。此外,较短的培养检测时间与较高的序贯器官衰竭评估评分相关,但与死亡率无关。
感染性休克患者常为培养阴性,尤其是感染部位在下呼吸道时。尽管培养阴性与一定程度的器官功能障碍相关,但它不是死亡的独立预测因素。