Department of Cardiology Amsterdam UMC, Vrije Universiteit AmsterdamAmsterdam Cardiovascular Sciences Amsterdam Netherlands.
Department of Cardiology Northwest Clinics Alkmaar The Netherlands.
J Am Heart Assoc. 2021 Apr 20;10(8):e019101. doi: 10.1161/JAHA.120.019101. Epub 2021 Apr 6.
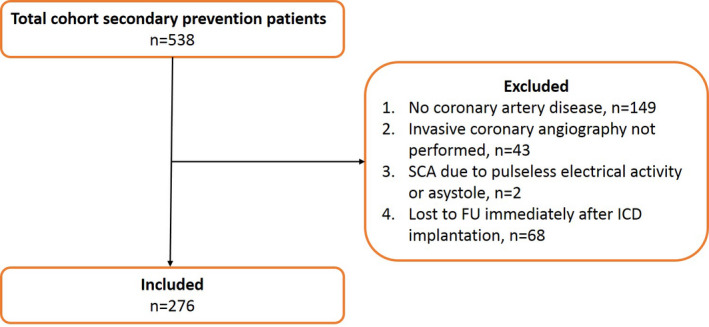
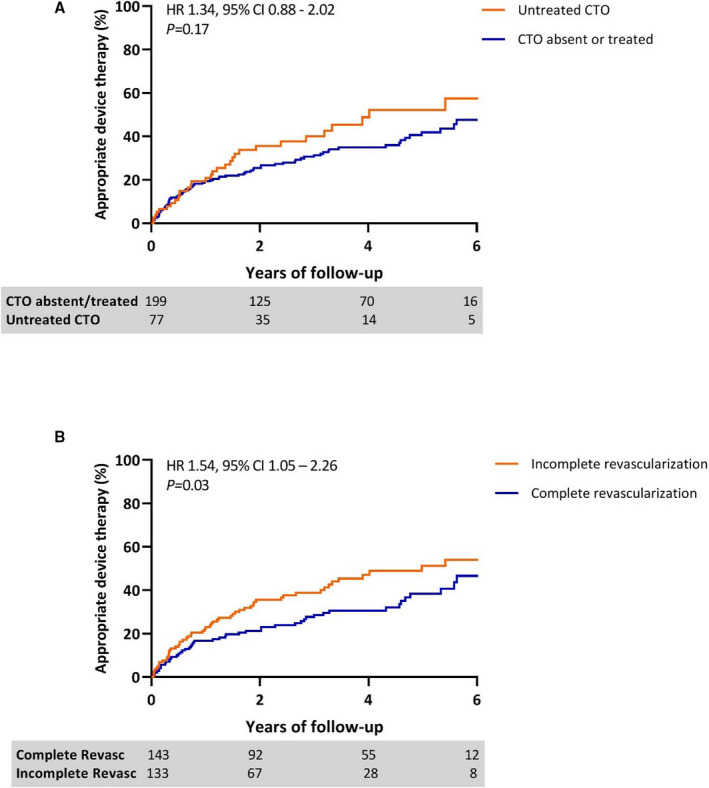
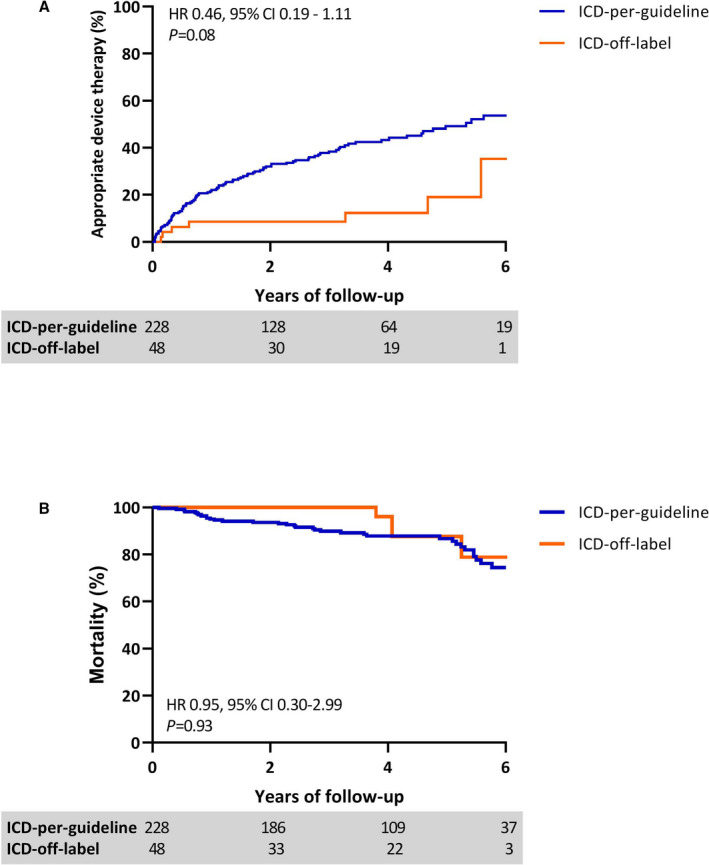
Background In survivors of sudden cardiac arrest with obstructive coronary artery disease, it remains challenging to distinguish ischemia as a reversible cause from irreversible scar-related ventricular arrhythmias. We aimed to evaluate the value of implantable cardioverter-defibrillator (ICD) implantation in sudden cardiac arrest survivors with presumably reversible ischemia and complete revascularization. Methods and Results This multicenter retrospective cohort study included 276 patients (80% men, age 67±10 years) receiving ICD implantation for secondary prevention. Angiography was performed before ICD implantation. A subgroup of 166 (60%) patients underwent cardiac magnetic resonance imaging with late gadolinium enhancement before implantation. Patients were divided in 2 groups, (1) ICD-per-guideline, including 228 patients with incomplete revascularization or left ventricular ejection fraction ≤35%, and (2) ICD-off-label, including 48 patients with complete revascularization and left ventricular ejection fraction >35%. The primary outcome was time to appropriate device therapy (ADT). During 4.0 years (interquartile range, 3.5-4.6) of follow-up, ADT developed in 15% of the ICD-off-label group versus 43% of the ICD-per-guideline group. Time to ADT was comparable in the ICD-off-label and ICD-per-guideline groups (hazard ratio (HR), 0.46; =0.08). No difference in mortality was observed (HR, 0.95; =0.93). Independent predictors of ADT included age (HR, 1.03; =0.01), left ventricular end-diastolic volume HR, (1.05 per 10 mL increase; <0.01) and extent of transmural late gadolinium enhancement (HR, 1.12; =0.04). Conclusions This study demonstrates that sudden cardiac arrest survivors with coronary artery disease remain at high risk of recurrent ventricular arrhythmia, even after complete revascularization and with preserved left ventricular function. Late gadolinium enhancement-cardiac magnetic resonance imaging derived left ventricular volumes and extent of myocardial scar were independently associated with.
背景 在伴有阻塞性冠状动脉疾病的心脏骤停幸存者中,区分缺血作为可逆性原因与不可逆性瘢痕相关室性心律失常仍然具有挑战性。我们旨在评估埋藏式心脏复律除颤器(ICD)植入对疑似可逆性缺血和完全血运重建的心脏骤停幸存者的价值。
方法和结果 这项多中心回顾性队列研究纳入了 276 名(80%为男性,年龄 67±10 岁)接受 ICD 植入二级预防的患者。在 ICD 植入前进行了血管造影。亚组的 166 名(60%)患者在植入前进行了心脏磁共振成像延迟钆增强检查。患者被分为 2 组,(1)ICD-指南,包括 228 名不完全血运重建或左心室射血分数≤35%的患者,和(2)ICD-标签外,包括 48 名完全血运重建和左心室射血分数>35%的患者。主要结局是适当的设备治疗(ADT)时间。在 4.0 年(四分位距 3.5-4.6)的随访期间,ICD-标签外组的 ADT 发生率为 15%,而 ICD-指南组为 43%。ICD-标签外和 ICD-指南组的 ADT 时间无差异(风险比(HR),0.46;=0.08)。未观察到死亡率差异(HR,0.95;=0.93)。ADT 的独立预测因素包括年龄(HR,1.03;=0.01)、左心室舒张末期容积(HR,每增加 10 毫升增加 1.05;<0.01)和透壁性延迟钆增强程度(HR,1.12;=0.04)。
结论 这项研究表明,即使在完全血运重建和保留左心室功能后,患有冠状动脉疾病的心脏骤停幸存者仍存在复发性室性心律失常的高风险。心脏磁共振成像衍生的左心室容积和心肌瘢痕程度与迟发性钆增强有关。