Raasveld Senta Jorinde, Delnoij Thijs S R, Broman Lars M, Lansink-Hartgring Annemieke Oude, Hermans Greet, De Troy Erwin, Taccone Fabio S, Diaz Manuel Quintana, der Velde Franciska van, Miranda Dinis Dos Reis, Scholten Erik, Vlaar Alexander P J
Department of Intensive Care, Amsterdam University Medical Centers, Location Academic Medical Center (26066AMC), Amsterdam, the Netherlands.
Department of Cardiology, 199236Maastricht University Medical Center, Maastricht, the Netherlands.
J Intensive Care Med. 2021 Aug;36(8):910-917. doi: 10.1177/08850666211007063. Epub 2021 Apr 7.
To report and compare the characteristics and outcomes of COVID-19 patients on extracorporeal membrane oxygenation (ECMO) to non-COVID-19 acute respiratory distress syndrome (ARDS) patients on ECMO.
We performed an international retrospective study of COVID-19 patients on ECMO from 13 intensive care units from March 1 to April 30, 2020. Demographic data, ECMO characteristics and clinical outcomes were collected. The primary outcome was to assess the complication rate and 28-day mortality; the secondary outcome was to compare patient and ECMO characteristics between COVID-19 patients on ECMO and non-COVID-19 related ARDS patients on ECMO (non-COVID-19; January 1, 2018 until July 31, 2019).
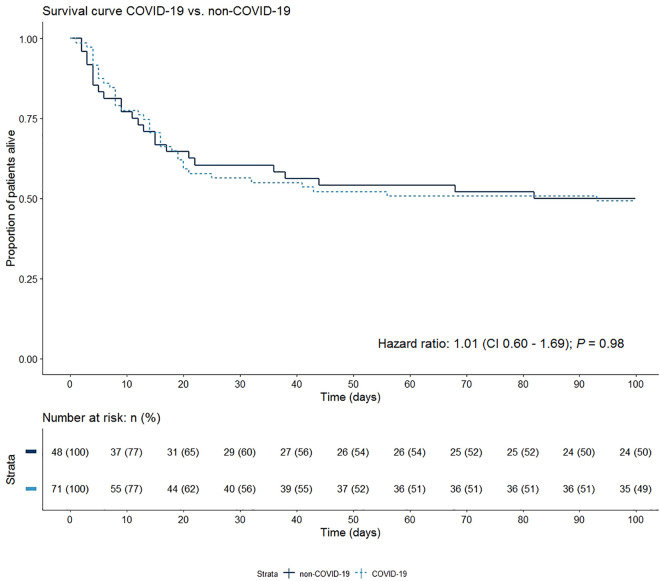
During the study period 71 COVID-19 patients received ECMO, mostly veno-venous, for a median duration of 13 days (IQR 7-20). ECMO was initiated at 5 days (IQR 3-10) following invasive mechanical ventilation. Median PaO/FiO ratio prior to initiation of ECMO was similar in COVID-19 patients (58 mmHg [IQR 46-76]) and non-COVID-19 patients (53 mmHg [IQR 44-66]), the latter consisting of 48 patients. 28-day mortality was 37% in COVID-19 patients and 27% in non-COVID-19 patients. However, Kaplan-Meier curves showed that after a 100-day follow-up this non-significant difference resolves. Non-surviving COVID-19 patients were more acidotic prior to initiation ECMO, had a shorter ECMO run and fewer received muscle paralysis compared to survivors.
No significant differences in outcomes were found between COVID-19 patients on ECMO and non-COVID-19 ARDS patients on ECMO. This suggests that ECMO could be considered as a supportive therapy in case of refractory respiratory failure in COVID-19.
报告并比较接受体外膜肺氧合(ECMO)治疗的新型冠状病毒肺炎(COVID-19)患者与接受ECMO治疗的非COVID-19急性呼吸窘迫综合征(ARDS)患者的特征及治疗结果。
我们对2020年3月1日至4月30日期间来自13个重症监护病房接受ECMO治疗的COVID-19患者进行了一项国际回顾性研究。收集了人口统计学数据、ECMO特征及临床结果。主要结局是评估并发症发生率和28天死亡率;次要结局是比较接受ECMO治疗的COVID-19患者与接受ECMO治疗的非COVID-19相关ARDS患者(非COVID-19;2018年1月1日至2019年7月31日)之间的患者及ECMO特征。
在研究期间,71例COVID-19患者接受了ECMO治疗,多数为静脉-静脉模式,中位治疗时间为13天(四分位间距7 - 20天)。ECMO在有创机械通气后5天(四分位间距3 - 10天)开始。COVID-19患者(58 mmHg [四分位间距46 - 76])和非COVID-19患者(53 mmHg [四分位间距44 - 66],后者48例)在开始ECMO治疗前的中位氧合指数相似。COVID-19患者的28天死亡率为37%,非COVID-19患者为27%。然而,Kaplan-Meier曲线显示,经过100天的随访,这种无显著差异的情况消失。与幸存者相比,未存活的COVID-19患者在开始ECMO治疗前酸中毒更严重,ECMO治疗时间更短,接受肌肉松弛治疗的更少。
接受ECMO治疗的COVID-19患者与接受ECMO治疗的非COVID-19 ARDS患者在治疗结果上未发现显著差异。这表明在COVID-19患者出现难治性呼吸衰竭时,ECMO可被视为一种支持性治疗方法。